The Primary Care Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge, United Kingdom.
Centre for Cancer Genetic Epidemiology, Department of Public Health and Primary Care, Strangeways Research Laboratory, Wort's Causeway, Cambridge, United Kingdom.
Cancer Prev Res (Phila). 2020 Jun;13(6):509-520. doi: 10.1158/1940-6207.CAPR-19-0521. Epub 2020 Feb 18.
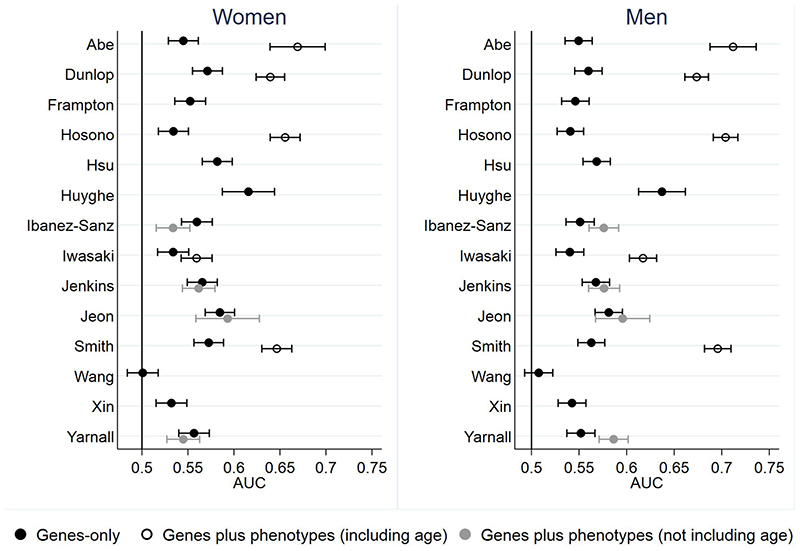
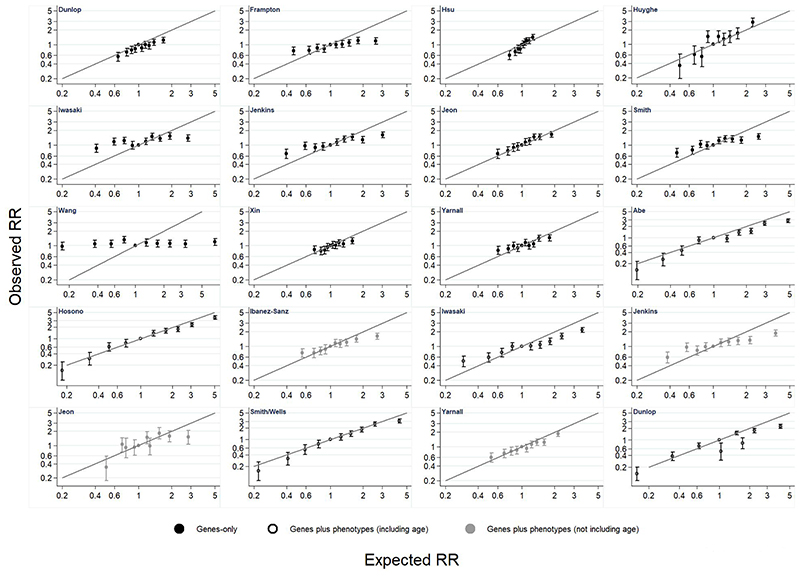
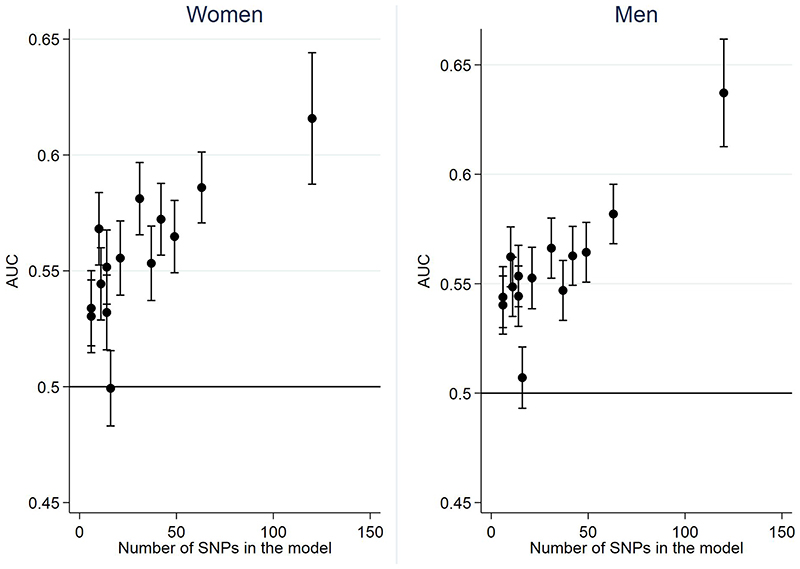
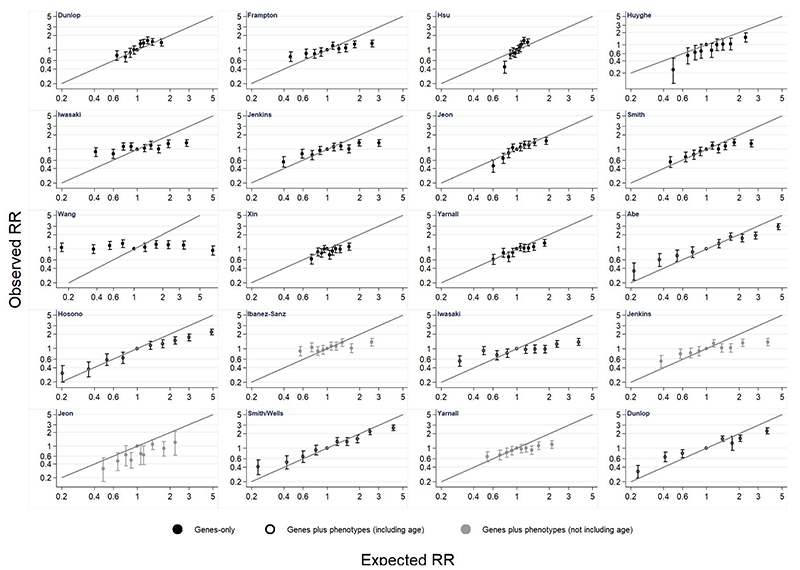
The aim of this study was to compare and externally validate risk scores developed to predict incident colorectal cancer that include common genetic variants (SNPs), with or without established lifestyle/environmental (questionnaire-based/classical/phenotypic) risk factors. We externally validated 23 risk models from a previous systematic review in 443,888 participants ages 37 to 73 from the UK Biobank cohort who had 6-year prospective follow-up, no prior history of colorectal cancer, and data for incidence of colorectal cancer through linkage to national cancer registries. There were 2,679 (0.6%) cases of incident colorectal cancer. We assessed model discrimination using the area under the operating characteristic curve (AUC) and relative risk calibration. The AUC of models including only SNPs increased with the number of included SNPs and was similar in men and women: the model by Huyghe with 120 SNPs had the highest AUC of 0.62 [95% confidence interval (CI), 0.59-0.64] in women and 0.64 (95% CI, 0.61-0.66) in men. Adding phenotypic risk factors without age improved discrimination in men but not in women. Adding phenotypic risk factors and age increased discrimination in all cases ( < 0.05), with the best performing models including SNPs, phenotypic risk factors, and age having AUCs between 0.64 and 0.67 in women and 0.67 and 0.71 in men. Relative risk calibration varied substantially across the models. Among middle-aged people in the UK, existing polygenic risk scores discriminate moderately well between those who do and do not develop colorectal cancer over 6 years. Consideration should be given to exploring the feasibility of incorporating genetic and lifestyle/environmental information in any future stratified colorectal cancer screening program.
本研究旨在比较和外部验证旨在预测结直肠癌发病风险的评分,这些评分包括常见的遗传变异(SNP),并结合或不结合已建立的生活方式/环境(问卷/经典/表型)风险因素。我们在 UK Biobank 队列中对来自先前系统评价的 23 种风险模型进行了外部验证,该队列包含年龄在 37 至 73 岁之间的 443888 名参与者,具有 6 年的前瞻性随访,无结直肠癌既往病史,通过与国家癌症登记处的数据链接,可获得结直肠癌的发病情况。有 2679 例(0.6%)结直肠癌发病。我们使用受试者工作特征曲线(AUC)下面积和相对风险校准来评估模型的区分度。仅包含 SNP 的模型的 AUC 随包含的 SNP 数量的增加而增加,且在男性和女性中相似:Huyghe 等人包含 120 个 SNP 的模型在女性中的 AUC 最高,为 0.62[95%置信区间(CI),0.59-0.64],在男性中为 0.64(95%CI,0.61-0.66)。在男性中,添加不包括年龄的表型风险因素可改善区分度,但在女性中则不然。在所有病例中添加表型风险因素和年龄均可提高区分度(<0.05),表现最佳的模型包括 SNP、表型风险因素和年龄,在女性中的 AUC 为 0.64 至 0.67,在男性中的 AUC 为 0.67 至 0.71。相对风险校准在各模型之间差异较大。在英国的中年人群中,现有的多基因风险评分在 6 年内较好地区分了那些患有和未患有结直肠癌的人群。应考虑探索将遗传和生活方式/环境信息纳入未来分层结直肠癌筛查计划的可行性。