Department I of Internal Medicine and Center of Integrated Oncology Aachen Bonn Cologne Duesseldorf, University of Cologne, Cologne, Germany.
Hopital Avicenne, Assistance Publique-Hopitaux de Paris (AP-HP), Service d'Hematologie Biologique, Bobigny, France.
Leukemia. 2020 Aug;34(8):2038-2050. doi: 10.1038/s41375-020-0747-7. Epub 2020 Feb 18.
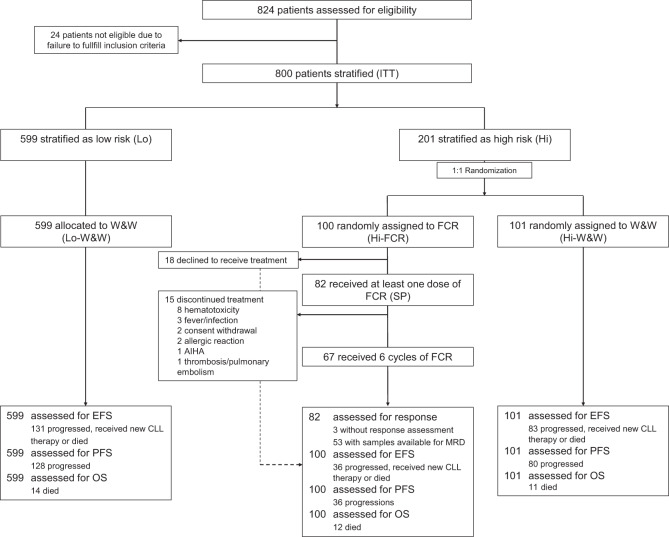
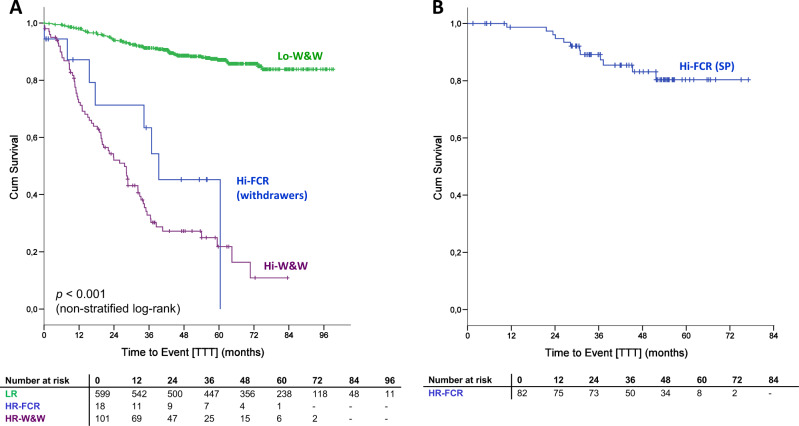
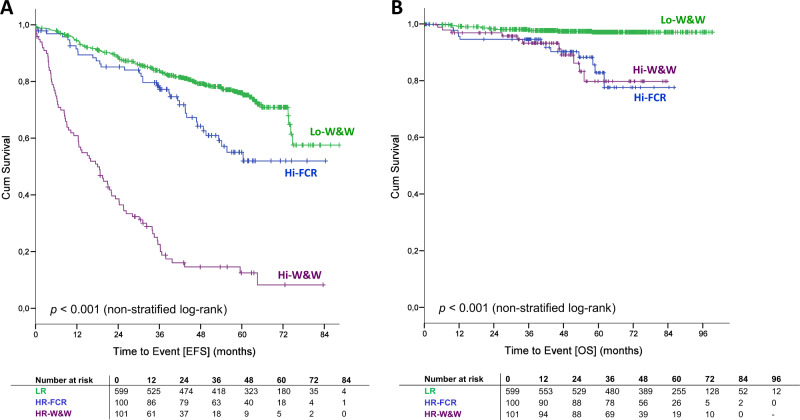
We report a randomized prospective phase 3 study (CLL7), designed to evaluate the efficacy of fludarabine, cyclophosphamide, and rituximab (FCR) in patients with an early-stage high-risk chronic lymphocytic leukemia (CLL). Eight hundred patients with untreated-stage Binet A disease were enrolled as intent-to-treat population and assessed for four prognostic markers: lymphocyte doubling time <12 months, serum thymidine kinase >10 U/L, unmutated IGHV genes, and unfavorable cytogenetics (del(11q)/del(17p)/trisomy 12). Two hundred and one patients with ≥2 risk features were classified as high-risk CLL and 1:1 randomized to receive either immediate therapy with 6xFCR (Hi-FCR, 100 patients), or to be observed according to standard of care (Hi-W&W, 101 patients). The overall response rate after early FCR was 92.7%. Common adverse events were hematological toxicities and infections (61.0%/41.5% of patients, respectively). After median observation time of 55.6 (0-99.2) months, event-free survival was significantly prolonged in Hi-FCR compared with Hi-W&W patients (median not reached vs. 18.5 months, p < 0.001). There was no significant overall survival benefit for high-risk patients receiving early FCR therapy (5-year OS 82.9% in Hi-FCR vs. 79.9% in Hi-W&W, p = 0.864). In conclusion, although FCR is efficient to induce remissions in the Binet A high-risk CLL, our data do not provide evidence that alters the current standard of care "watch and wait" for these patients.
我们报告了一项随机前瞻性 3 期研究(CLL7),旨在评估氟达拉滨、环磷酰胺和利妥昔单抗(FCR)在早期高危慢性淋巴细胞白血病(CLL)患者中的疗效。800 名未经治疗的 Binet A 期疾病患者被纳入意向治疗人群,并评估了四个预后标志物:淋巴细胞倍增时间<12 个月、血清胸苷激酶>10U/L、未突变 IGHV 基因和不良细胞遗传学(del(11q)/del(17p)/三体 12)。201 名≥2 个风险特征的患者被归类为高危 CLL,并以 1:1 的比例随机分为立即接受 6xFCR 治疗(Hi-FCR,100 名患者)或根据标准护理进行观察(Hi-W&W,101 名患者)。早期 FCR 后的总体缓解率为 92.7%。常见的不良反应是血液学毒性和感染(分别为 61.0%/41.5%的患者)。在 55.6(0-99.2)个月的中位观察时间后,与 Hi-W&W 患者相比,Hi-FCR 患者的无事件生存显著延长(中位未达到 vs. 18.5 个月,p<0.001)。接受早期 FCR 治疗的高危患者没有显著的总体生存获益(Hi-FCR 患者的 5 年 OS 为 82.9%,Hi-W&W 患者为 79.9%,p=0.864)。总之,尽管 FCR 能有效诱导 Binet A 期高危 CLL 缓解,但我们的数据并未提供证据表明改变目前对这些患者的“观察等待”标准护理。