Department of Epidemiology, Milken Institute School of Public Health, George Washington University, Washington, DC.
Emory Global Diabetes Research Center, Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, Georgia.
JAMA Netw Open. 2020 Feb 5;3(2):e1921618. doi: 10.1001/jamanetworkopen.2019.21618.
Antihypertension medications have been associated with prevention of cardiovascular events, although less is known about the comparative effectiveness of different medication classes.
To compare contemporary aggregated first-in-trial cardiovascular events among patients with hypertension and no substantial comorbidities.
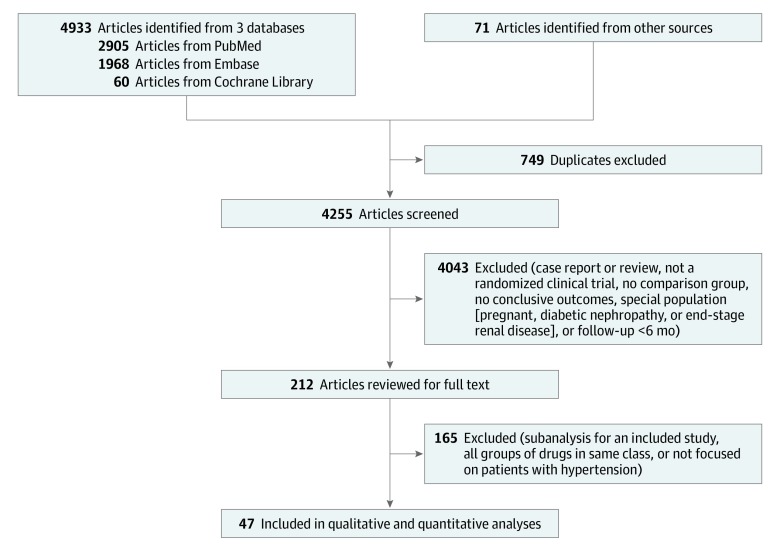
The PubMed, Embase, and Cochrane Library databases were systematically searched for articles published between January 1, 1990, and October 24, 2017.
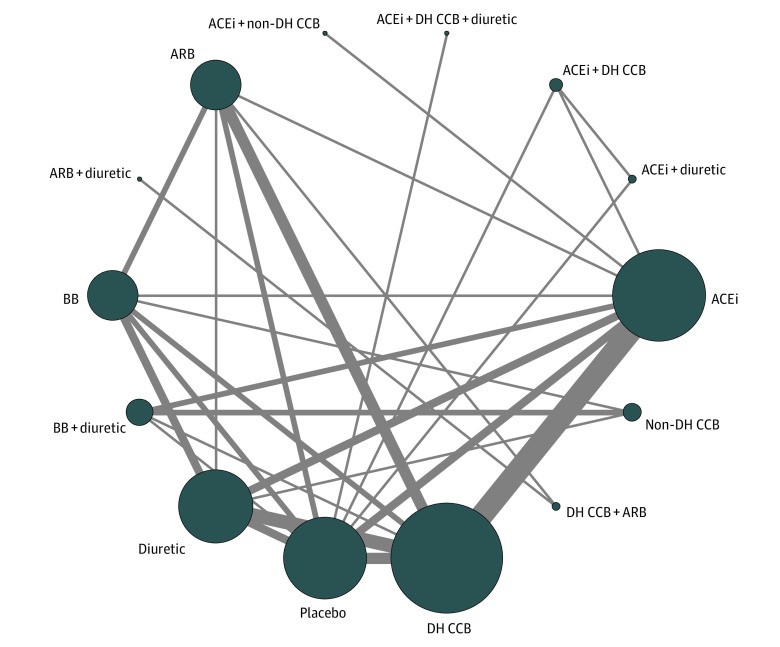
Randomized clinical trials that tested commonly used antihypertension medications (angiotensin-converting enzyme inhibitors, dihydropyridine calcium channel blockers, nondihydropyridine calcium channel blockers, β-blockers, angiotensin receptor blockers, and diuretics) and that reported selected cardiovascular outcomes for at least 6 months of follow-up.
The analysis was conducted from October 2017 to December 2019. Two reviewers extracted the number of cardiovascular events at the end of treatment for all study groups. For each outcome, a frequentist network meta-analysis was used to compare risk reductions between medication classes (random-effects models weighted by the inverse variance). The dose-response association between a 10-mm Hg reduction of systolic blood pressure and a 5-mm Hg reduction of diastolic blood pressure and the risk of first-in-trial cardiovascular events was estimated.
First-in-trial cardiovascular events, including cardiovascular death, myocardial infarction, stroke, and revascularization.
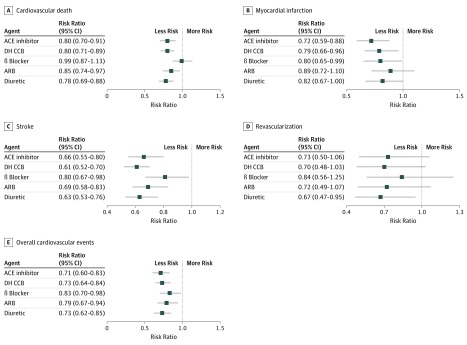
In this systematic review and network meta-analysis, data were pooled from 46 eligible clinical trials (248 887 total participants with a mean [SD] age of 65.6 [5.8] years; 52.8% men). In the network meta-analysis, compared with placebo, angiotensin-converting enzyme inhibitors, dihydropyridine calcium channel blockers, and thiazide diuretics were reported to be similarly effective in reducing overall cardiovascular events (25%), cardiovascular death (20%), and stroke (35%); angiotensin-converting enzyme inhibitors were reported to be the most effective in reducing the risk of myocardial infarction (28%); and diuretics were reported to be the most effective in reducing revascularization (33%). In the metaregression analyses, each 10-mm Hg reduction in systolic blood pressure and 5-mm Hg reduction in diastolic blood pressure was significantly associated with a lower risk of cardiovascular death, stroke, and overall cardiovascular events.
In this network meta-analysis of clinical trials of patients with hypertension and no substantial comorbidities, different classes of antihypertension medications were associated with similar benefits in reducing cardiovascular events. Future studies should compare the effectiveness of combinations of antihypertension medications in reducing cardiovascular events.
抗高血压药物与预防心血管事件有关,尽管对于不同药物类别的比较有效性知之甚少。
比较无明显合并症的高血压患者的第一代临床试验中综合心血管事件。
系统地检索了 1990 年 1 月 1 日至 2017 年 10 月 24 日期间发表在 PubMed、Embase 和 Cochrane 图书馆数据库中的文章。
随机临床试验,测试常用的抗高血压药物(血管紧张素转换酶抑制剂、二氢吡啶钙通道阻滞剂、非二氢吡啶钙通道阻滞剂、β受体阻滞剂、血管紧张素受体阻滞剂和利尿剂),并报告至少 6 个月随访的选定心血管结局。
分析于 2017 年 10 月至 2019 年 12 月进行。两名审查员提取了所有研究组治疗结束时心血管事件的数量。对于每个结局,使用随机效应模型(加权反比方差)比较药物类别的风险降低。还估计了收缩压降低 10mmHg 和舒张压降低 5mmHg 与第一代心血管事件风险之间的剂量-反应关联。
第一代心血管事件,包括心血管死亡、心肌梗死、中风和血运重建。
在这项系统评价和网络荟萃分析中,从 46 项合格的临床试验中汇总了数据(共有 248887 名参与者,平均年龄[标准差]为 65.6[5.8]岁;52.8%为男性)。在网络荟萃分析中,与安慰剂相比,血管紧张素转换酶抑制剂、二氢吡啶钙通道阻滞剂和噻嗪类利尿剂在降低整体心血管事件(25%)、心血管死亡(20%)和中风(35%)方面同样有效;血管紧张素转换酶抑制剂在降低心肌梗死风险方面最为有效(28%);利尿剂在降低血运重建风险方面最为有效(33%)。在荟萃回归分析中,收缩压每降低 10mmHg 和舒张压每降低 5mmHg 与心血管死亡、中风和整体心血管事件的风险降低显著相关。
在这项无明显合并症的高血压患者临床试验的网络荟萃分析中,不同类别的抗高血压药物在降低心血管事件方面具有相似的益处。未来的研究应比较抗高血压药物联合使用在降低心血管事件方面的有效性。