Department of Urology, University Hospital Schleswig-Holstein, Campus Luebeck, Ratzeburger Allee 160, 23538, Luebeck, Germany.
Department of Urology, Medical School Hannover, Carl-Neuberg-Strasse 1, 30265, Hannover, Germany.
BMC Cancer. 2020 Feb 21;20(1):140. doi: 10.1186/s12885-020-6620-2.
Whether or not double J (DJ) stenting during transurethral resection of a bladder tumour (TURBT) harms patients with regard to possible metachronous upper urinary tract urothelial cancer (UUTUC) development remains controversial. This study evaluated the impact of DJ compared to nephrostomy placement during TURBT for bladder cancer (BCa) on the incidence of metachronous UUTUCs.
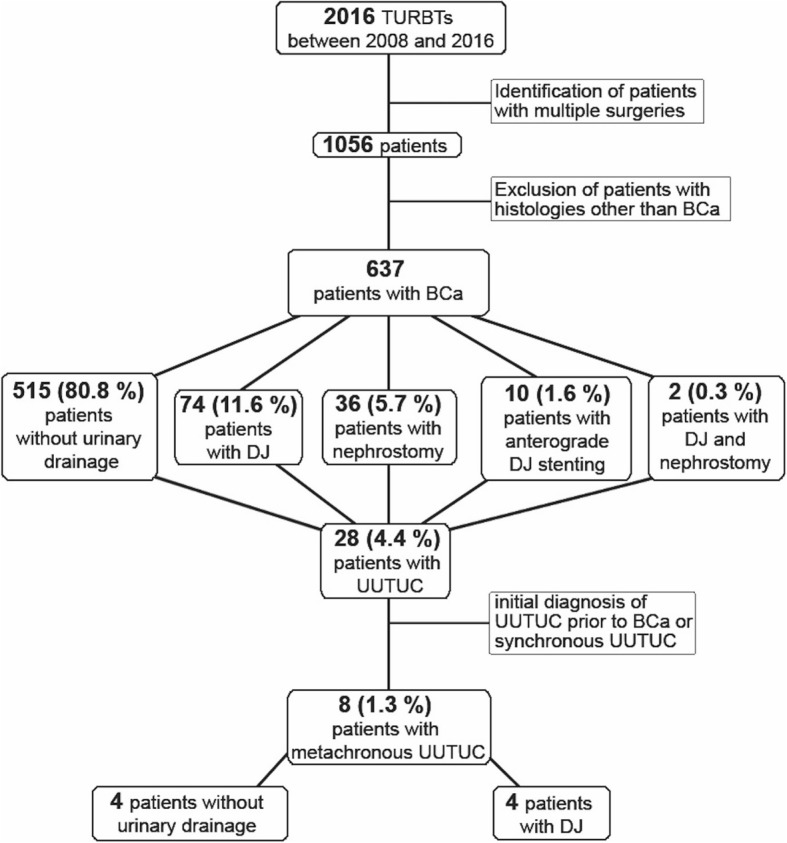
We retrospectively analysed 637 patients who underwent TURBT in our department between 2008 and 2016. BCa, UUTUC and urinary drainage data (retrograde/anterograde DJ and percutaneous nephrostomy) were assessed, along with the prevalence of hydronephrosis, and mortality. Chi-square and Fisher's exact test was performed for univariate analyses. Survival analysis was performed by the Kaplan-Meier method and log-rank tests.
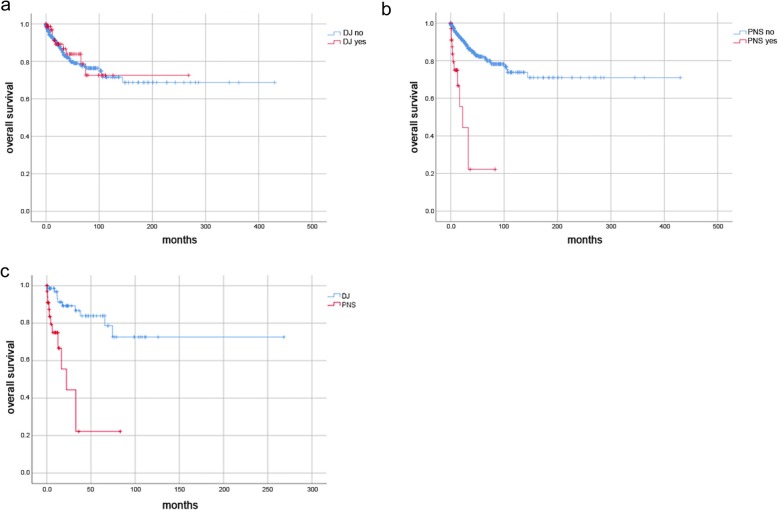
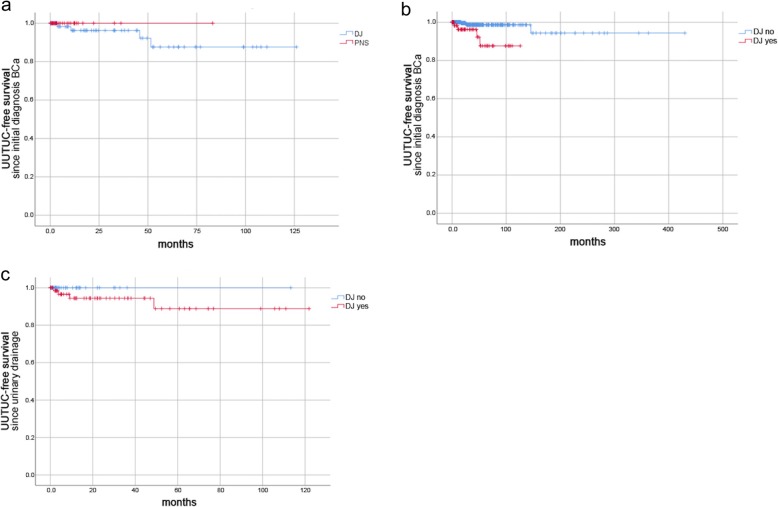
UUTUC was noted in 28 out of 637 patients (4.4%), whereas only eight (1.3%) developed it metachronously to BCa. Out of these, four patients received DJ stents, while four patients received no urinary drainage of the upper urinary tract. Placement of urinary drainage significantly correlated with UUTUC (50.0% vs. 17.9%; p = 0.041). DJ stenting significantly correlated with UUTUC (50.0% vs. 11%; p < 0.01), while no patient with a nephrostomy tube developed UUTUC. UUTUC-free survival rates were significantly lower for patients with DJ stents than for all other patients (p = 0.001). Patients with or without DJ stents had similar overall survival (OS) rates (p = 0.73), whereas patients with nephrostomy tubes had significantly lower OS rates than all other patients (p < 0.001).
Patients with DJ stenting during TURBT for BCa might have an increased risk of developing metachronous UUTUC. This study indicated advantages in placing nephrostomy tubes rather than DJ stents; however, confirmation requires investigation of a larger cohort. Even so, the increased mortality rate in the nephrostomy group reflected hydronephrosis as an unfavourable prognostic factor.
经尿道膀胱肿瘤切除术(TURBT)期间是否放置双 J(DJ)支架对可能发生的上尿路上皮癌(UUTUC)的发展是否有害仍存在争议。本研究评估了与 TURBT 期间放置肾造瘘管相比,DJ 支架对膀胱癌(BCa)患者 UUTUC 发生率的影响。
我们回顾性分析了 2008 年至 2016 年期间在我科接受 TURBT 的 637 例患者。评估了 BCa、UUTUC 和尿引流数据(逆行/顺行 DJ 和经皮肾造瘘),以及肾积水的发生率和死亡率。进行了卡方和 Fisher 确切检验进行单变量分析。通过 Kaplan-Meier 方法和对数秩检验进行生存分析。
637 例患者中有 28 例(4.4%)出现 UUTUC,其中仅 8 例(1.3%)为膀胱癌后发生。其中 4 例接受了 DJ 支架,4 例未进行上尿路尿引流。尿引流的放置与 UUTUC 显著相关(50.0% vs. 17.9%;p=0.041)。DJ 支架与 UUTUC 显著相关(50.0% vs. 11%;p<0.01),而无患者因放置肾造瘘管而发生 UUTUC。与其他患者相比,放置 DJ 支架的患者 UUTUC 无复发生存率显著较低(p=0.001)。有或没有 DJ 支架的患者总生存率(OS)相似(p=0.73),而有肾造瘘管的患者 OS 显著低于其他患者(p<0.001)。
在 TURBT 治疗 BCa 期间放置 DJ 支架的患者可能有发生上尿路上皮癌的风险增加。本研究表明,放置肾造瘘管优于 DJ 支架;然而,这需要更大的队列研究来证实。即便如此,肾造瘘组的死亡率增加反映了肾积水是一个不利的预后因素。