Department of Paediatrics, School of Medicine, University of Washington, Seattle, WA, USA; Division of Pulmonary and Sleep Medicine, Seattle Children's Hospital, Seattle, WA, USA.
Division of Pulmonary and Critical Care, Johns Hopkins University School of Medicine, Baltimore, MD, USA; Centre for Global Non-Communicable Disease Research and Training, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Lancet Glob Health. 2020 Mar;8(3):e362-e373. doi: 10.1016/S2214-109X(19)30543-1.
In resource-limited settings, pneumonia diagnosis and management are based on thresholds for respiratory rate (RR) and oxyhaemoglobin saturation (SpO) recommended by WHO. However, as RR increases and SpO decreases with elevation, these thresholds might not be applicable at all altitudes. We sought to determine upper thresholds for RR and lower thresholds for SpO by age and altitude at four sites, with altitudes ranging from sea level to 4348 m.
In this cross-sectional study, we enrolled healthy children aged 0-23 months who lived within the study areas in India, Guatemala, Rwanda, and Peru. Participants were excluded if they had been born prematurely (<37 weeks gestation); had a congenital heart defect; had history in the past 2 weeks of overnight admission to a health facility, diagnosis of pneumonia, antibiotic use, or respiratory or gastrointestinal signs; history in the past 24 h of difficulty breathing, fast breathing, runny nose, or nasal congestion; and current runny nose, nasal congestion, fever, chest indrawing, or cyanosis. We measured RR either automatically with the Masimo Rad-97, manually, or both, and measured SpO with the Rad-97. Trained staff measured RR in duplicate and SpO in triplicate in children who had no respiratory symptoms or signs in the past 2 weeks. We estimated smooth percentiles for RR and SpO that varied by age and site using generalised additive models for location, shape, and scale. We compared these data with WHO RR and SpO thresholds for tachypnoea and hypoxaemia to determine agreement.
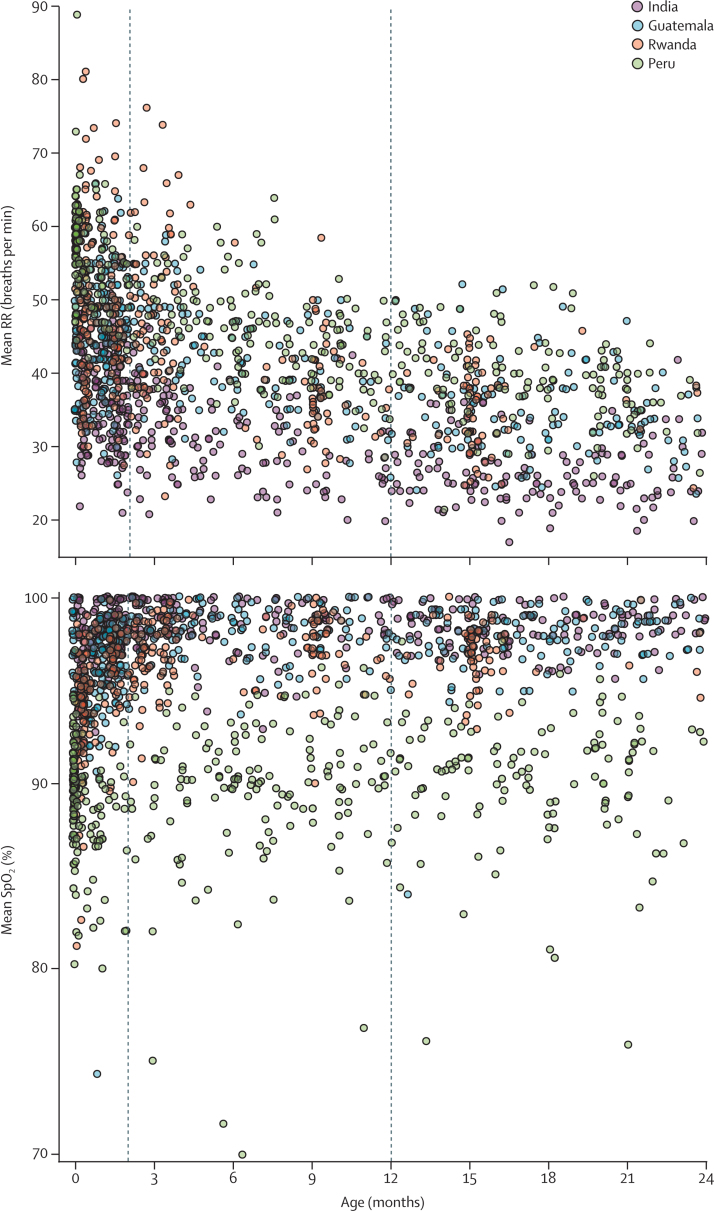
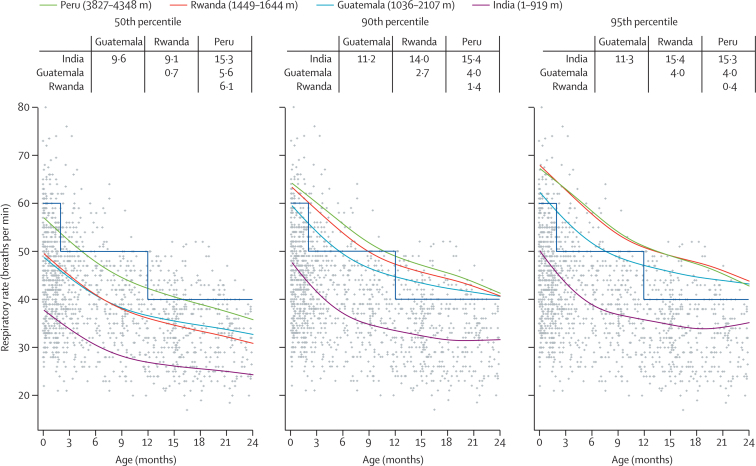
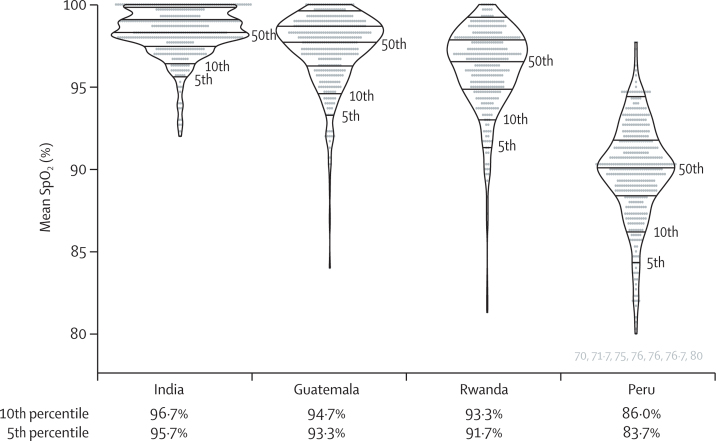
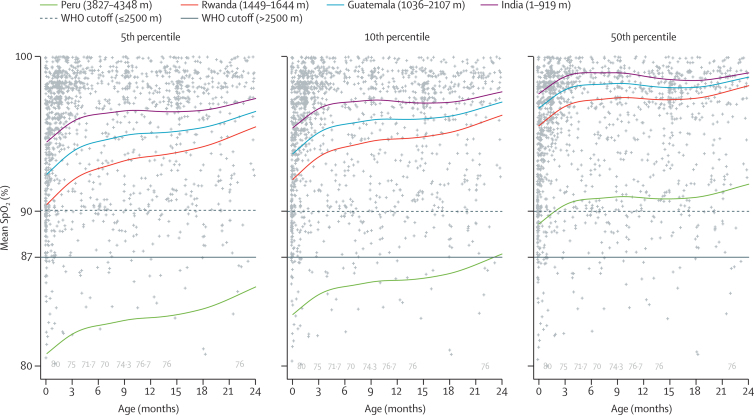
Between Nov 24, 2017, and Oct 10, 2018, we screened 2027 children for eligibility. 335 were ineligible, leaving 1692 eligible participants. 30 children were excluded because of missing values and 92 were excluded because of measurement or data entry errors, leaving 1570 children in the final analysis. 404 participants were from India (altitude 1-919 m), 389 were from Guatemala (1036-2017 m), 341 from Rwanda (1449-1644 m), and 436 from Peru (3827-4348 m). Mean age was 7·2 months (SD 7·2) and 796 (50·7%) of 1570 participants were female. Although average age was mostly similar between settings, the average participant age in Rwanda was noticeably younger, at 5·5 months (5·9). In the 1570 children included in the analysis, mean RR was 31·9 breaths per min (SD 7·1) in India, 41·5 breaths per min in Guatemala (8·4), 44·0 breaths per min in Rwanda (10·8), and 48·0 breaths per min in Peru (9·4). Mean SpO was 98·3% in India (SD 1·5), 97·3% in Guatemala (2·4), 96·2% in Rwanda (2·6), and 89·7% in Peru (3·5). Compared to India, mean RR was 9·6 breaths per min higher in Guatemala, 12·1 breaths per min higher in Rwanda, and 16·1 breaths per min higher in Peru (likelihood ratio test p<0·0001). Smooth percentiles for RR and SpO varied by site and age. When we compared age-specific and site-specific 95th percentiles for RR and 5th percentiles for SpO against the WHO cutoffs, we found that the proportion of false positives for tachypnoea increased with altitude: 0% in India (95% CI 0-0), 7·3% in Guatemala (4·1-10·4), 16·8% in Rwanda (12·9-21·1), and 28·9% in Peru (23·7-33·0). We also found a high proportion of false positives for hypoxaemia in Peru (11·6%, 95% CI 7·0-14·7).
WHO cutoffs for fast breathing and hypoxaemia overlap with RR and SpO values that are normal for children in different altitudes. Use of WHO definitions for fast breathing could result in misclassification of pneumonia in many children who live at moderate to high altitudes and show acute respiratory signs. The 5th percentile for SpO was in reasonable agreement with the WHO definition of hypoxaemia in all regions except for Peru (the highest altitude site). Misclassifications could result in inappropriate management of paediatric respiratory illness and misdirection of potentially scarce resources such as antibiotics and supplemental oxygen. Future studies at various altitudes are needed to validate our findings and recommend a revision to current guidelines. Substantiating research in sick children is still needed.
US National Institutes of Health, Bill & Melinda Gates Foundation.
在资源有限的情况下,肺炎的诊断和管理基于世界卫生组织(WHO)推荐的呼吸频率(RR)和血氧饱和度(SpO)阈值。然而,随着海拔的升高,RR 增加,SpO 降低,这些阈值可能并不适用于所有海拔高度。我们旨在确定四个地点(海拔范围从海平面到 4348 米)按年龄和海拔划分的 RR 上限和 SpO 下限。
在这项横断面研究中,我们招募了居住在印度、危地马拉、卢旺达和秘鲁研究区域内 0-23 个月龄的健康儿童。如果儿童有以下情况则被排除在外:早产(<37 周妊娠);先天性心脏病;过去 2 周内有过夜间住院、肺炎诊断、抗生素使用或呼吸或胃肠道症状的病史;过去 24 小时内有呼吸困难、呼吸急促、流鼻涕或鼻塞的病史;目前有流鼻涕、鼻塞、发热、胸部凹陷或发绀。我们使用 Masimo Rad-97 自动或手动测量 RR,并用 Rad-97 测量 SpO。在过去 2 周内没有出现呼吸道症状或体征的儿童中,由经过培训的工作人员重复测量 RR,用三重测量 SpO。使用位置、形状和比例的广义加性模型来估计 RR 和 SpO 的平滑百分位数,这些百分位数随年龄和地点而变化。我们将这些数据与 WHO 用于确定呼吸急促和低氧血症的 RR 和 SpO 阈值进行比较,以确定一致性。
在 2017 年 11 月 24 日至 2018 年 10 月 10 日期间,我们对 2027 名儿童进行了筛选,以确定其是否符合纳入标准。其中 335 名儿童不符合条件,其余 1692 名儿童符合条件。有 30 名儿童因数据缺失被排除,92 名儿童因测量或数据输入错误被排除,最终有 1570 名儿童纳入分析。其中 404 名儿童来自印度(海拔 1-919 米),389 名儿童来自危地马拉(海拔 1036-2017 米),341 名儿童来自卢旺达(海拔 1449-1644 米),436 名儿童来自秘鲁(海拔 3827-4348 米)。平均年龄为 7.2 个月(SD 7.2),1570 名参与者中 796 名(50.7%)为女性。虽然各地区的平均年龄大致相似,但卢旺达的平均参与者年龄明显较小,为 5.5 个月(5.9)。在纳入分析的 1570 名儿童中,RR 的平均值在印度为 31.9 次/分钟(SD 7.1),在危地马拉为 41.5 次/分钟(8.4),在卢旺达为 44.0 次/分钟(10.8),在秘鲁为 48.0 次/分钟(9.4)。SpO 的平均值在印度为 98.3%(SD 1.5),在危地马拉为 97.3%(2.4),在卢旺达为 96.2%(2.6),在秘鲁为 89.7%(3.5)。与印度相比,危地马拉 RR 平均高 9.6 次/分钟,卢旺达 RR 平均高 12.1 次/分钟,秘鲁 RR 平均高 16.1 次/分钟(似然比检验 p<0.0001)。RR 和 SpO 的平滑百分位数随地点和年龄而变化。当我们比较 RR 的年龄特异性和地点特异性 95%百分位数和 SpO 的 5%百分位数与 WHO 截止值时,我们发现随着海拔的升高,呼吸急促的假阳性比例增加:印度为 0%(95%CI 0-0),危地马拉为 7.3%(4.1-10.4),卢旺达为 16.8%(12.9-21.1),秘鲁为 28.9%(23.7-33.0)。我们还发现秘鲁低氧血症的假阳性比例很高(11.6%,95%CI 7.0-14.7)。
WHO 用于呼吸急促和低氧血症的截止值与不同海拔高度儿童的正常 RR 和 SpO 值重叠。在许多居住在中高度海拔地区并出现急性呼吸道症状的儿童中,使用 WHO 定义的快速呼吸可能会导致肺炎的误诊。SpO 的第 5 百分位与所有地区(除了海拔最高的秘鲁地区)的 WHO 低氧血症定义大致一致。除了秘鲁(海拔最高的地点)之外,在所有地区,SpO 的第 5 百分位与 WHO 定义的低氧血症在分类上具有良好的一致性。在秘鲁,SpO 的第 5 百分位与 WHO 定义的低氧血症之间存在差异,可能是因为海拔较高的地区,SpO 降低,但仍在第 5 百分位范围内。分类错误可能导致对儿科呼吸道疾病的不适当管理,以及对潜在稀缺资源(如抗生素和补充氧气)的错误分配。需要在不同海拔高度进行进一步的研究,以验证我们的发现并建议修订当前的指南。在患病儿童中进行的研究仍然是必要的。
美国国立卫生研究院,比尔和梅琳达·盖茨基金会。