From the Global Program in Pediatric Respiratory Sciences, Eudowood Division of Pediatric Respiratory Sciences (E.D.M.), the Division of Pulmonary and Critical Care (S.H., S.M.S., D.G.-P., S.M.H., K.N.W., L.N., W.C.), and the Center for Global Non-Communicable Disease Research and Training, School of Medicine (S.H., S.M.S., D.G.-P., S.M.H., K.N.W., L.N., W.C.), and the Department of International Health (E.D.M.) and the Program in Global Disease Epidemiology and Control, Department of International Health (L.H.M.), Bloomberg School of Public Health, Johns Hopkins University, Baltimore, the Division of Healthcare Delivery Research, MedStar Health Research Institute, Hyattsville (S.M.S.), and Fogarty International Center, National Institutes of Health, Bethesda (J.P.R.) - all in Maryland; the Global Health Institute, Department of Epidemiology and Biostatistics (J.P.M., L.M.G.), and the Department of Environmental Health Science, College of Public Health (L.P.N.), University of Georgia, Athens, and the Department of Biostatistics and Bioinformatics (H.H.C., L.A.W., S.J., J.W., Y.C.) and the Gangarosa Department of Environmental Health (A.E.L., K.S., T.F.C.), Rollins School of Public Health, and the Nell Hodgson Woodruff School of Nursing (L.M.T.), Emory University, Atlanta - both in Georgia; the Center for Health Studies, Universidad del Valle de Guatemala, Guatemala City (J.P.M., L.M.G., A.C., A.D.-A.); the Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston (M.A.K.); the Division of Pulmonary and Critical Care Medicine, Georgetown University, Washington DC (S.M.S.); the Department of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London (G.R.), and Nuffield Department of Women's and Reproductive Health, University of Oxford, Oxford (A.T.P.) - both in the United Kingdom; Eagle Research Center, Kigali, Rwanda (A.M.); the Indian Council of Medical Research Center for Advanced Research on Air Quality, Climate and Health, Department of Environmental Health Engineering, Sri Ramachandra Institute for Higher Education and Research, Chennai, India (K.B., G.T., S.S.G.); the Global Health Center, Institute for Public Health and Cardiovascular Division, Department of Medicine, Washington University, St. Louis, MO (V.G.D.-R., L.J.U.); the Division of Environmental Health Sciences, School of Public Health, University of California, Berkeley (A.P., W.Y.), and Berkeley Air Monitoring Group (M.A.J.) - both in Berkeley, CA; and the Department of Environmental and Radiological Health Sciences, Colorado State University, Fort Collins (J.L.P.).
N Engl J Med. 2024 Jan 4;390(1):32-43. doi: 10.1056/NEJMoa2305681.
Exposure to household air pollution is a risk factor for severe pneumonia. The effect of replacing biomass cookstoves with liquefied petroleum gas (LPG) cookstoves on the incidence of severe infant pneumonia is uncertain.
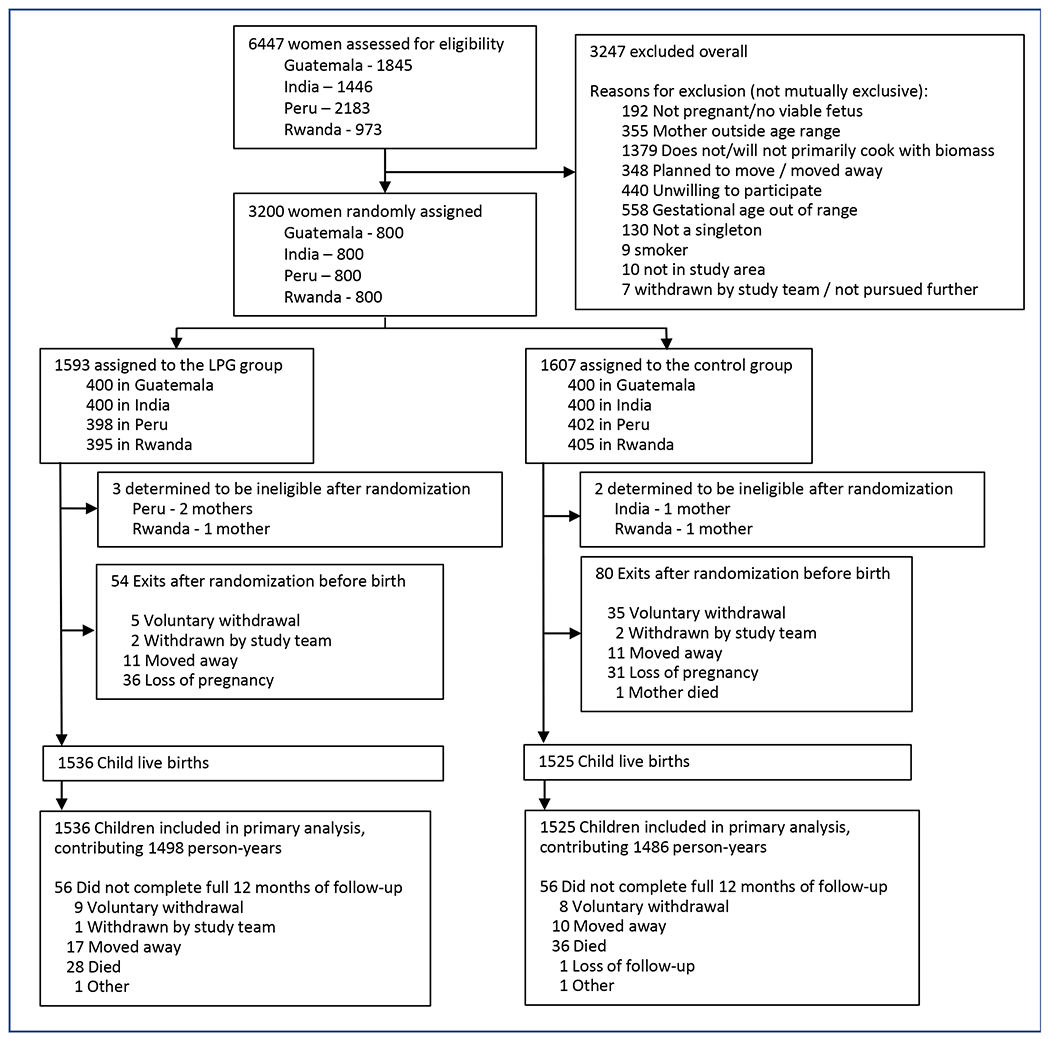
We conducted a randomized, controlled trial involving pregnant women 18 to 34 years of age and between 9 to less than 20 weeks' gestation in India, Guatemala, Peru, and Rwanda from May 2018 through September 2021. The women were assigned to cook with unvented LPG stoves and fuel (intervention group) or to continue cooking with biomass fuel (control group). In each trial group, we monitored adherence to the use of the assigned cookstove and measured 24-hour personal exposure to fine particulate matter (particles with an aerodynamic diameter of ≤2.5 μm [PM]) in the women and their offspring. The trial had four primary outcomes; the primary outcome for which data are presented in the current report was severe pneumonia in the first year of life, as identified through facility surveillance or on verbal autopsy.
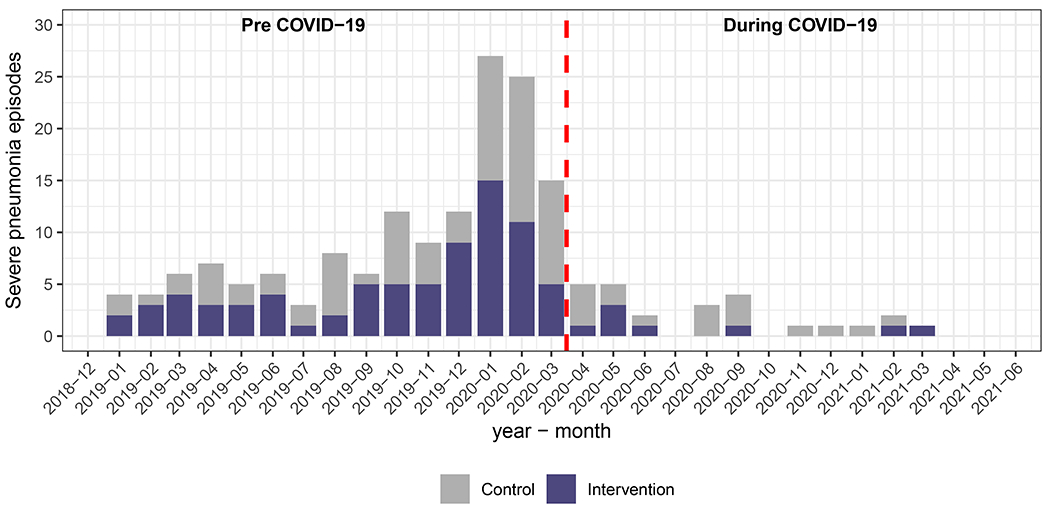
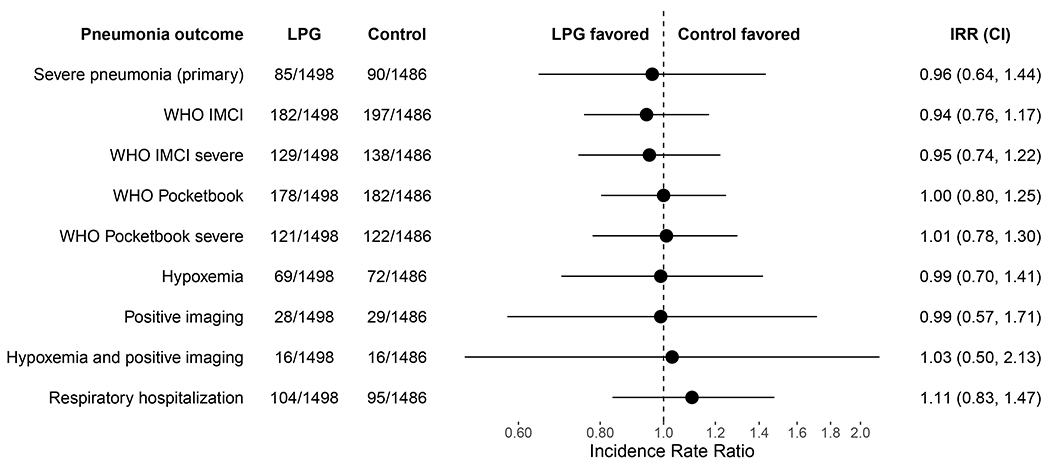
Among 3200 pregnant women who had undergone randomization, 3195 remained eligible and gave birth to 3061 infants (1536 in the intervention group and 1525 in the control group). High uptake of the intervention led to a reduction in personal exposure to PM among the children, with a median exposure of 24.2 μg per cubic meter (interquartile range, 17.8 to 36.4) in the intervention group and 66.0 μg per cubic meter (interquartile range, 35.2 to 132.0) in the control group. A total of 175 episodes of severe pneumonia were identified during the first year of life, with an incidence of 5.67 cases per 100 child-years (95% confidence interval [CI], 4.55 to 7.07) in the intervention group and 6.06 cases per 100 child-years (95% CI, 4.81 to 7.62) in the control group (incidence rate ratio, 0.96; 98.75% CI, 0.64 to 1.44; P = 0.81). No severe adverse events were reported to be associated with the intervention, as determined by the trial investigators.
The incidence of severe pneumonia among infants did not differ significantly between those whose mothers were assigned to cook with LPG stoves and fuel and those whose mothers were assigned to continue cooking with biomass stoves. (Funded by the National Institutes of Health and the Bill and Melinda Gates Foundation; HAPIN ClinicalTrials.gov number, NCT02944682.).
暴露于家庭空气污染是导致严重肺炎的一个风险因素。用液化石油气 (LPG) 炉具替代生物质燃料炉具对婴儿严重肺炎发病率的影响尚不确定。
我们在印度、危地马拉、秘鲁和卢旺达进行了一项随机、对照试验,纳入年龄在 18 至 34 岁之间、妊娠 9 周至不足 20 周的孕妇。这些妇女被分配使用无通风的 LPG 炉具和燃料(干预组)或继续使用生物质燃料烹饪(对照组)。在每个试验组中,我们监测了对指定炉具使用的依从性,并测量了妇女及其后代的 24 小时个人细颗粒物(空气动力学直径≤2.5μm 的颗粒[PM])暴露量。该试验有四个主要结局;本报告介绍的数据是婴儿生命第一年的严重肺炎,这是通过设施监测或口头尸检确定的。
在 3200 名接受随机分组的孕妇中,有 3195 名符合条件并分娩了 3061 名婴儿(干预组 1536 名,对照组 1525 名)。高比例的妇女参与干预措施导致儿童的 PM 个人暴露量减少,干预组中位数暴露量为每立方米 24.2μg(四分位距,17.8 至 36.4),对照组中位数暴露量为每立方米 66.0μg(四分位距,35.2 至 132.0)。在婴儿生命的第一年中,共发现 175 例严重肺炎病例,干预组每 100 名儿童年发病率为 5.67 例(95%置信区间[CI],4.55 至 7.07),对照组为 6.06 例(95%CI,4.81 至 7.62)(发病率比,0.96;98.75%CI,0.64 至 1.44;P=0.81)。试验调查人员确定,没有报告与干预相关的严重不良事件。
与母亲被分配使用生物质燃料炉具的婴儿相比,母亲被分配使用液化石油气炉具和燃料的婴儿的严重肺炎发病率无显著差异。(由美国国立卫生研究院和比尔及梅琳达·盖茨基金会资助;HAPIN 临床试验.gov 编号,NCT02944682。)