Merkel Peter A, Jayne David R, Wang Chao, Hillson Jan, Bekker Pirow
Division of Rheumatology, Department of Medicine, University of Pennsylvania, Philadelphia, PA, United States.
Division of Clinical Epidemiology, Department of Biostatistics, Epidemiology, and Informatics, University of Pennsylvania, Philadelphia, PA, United States.
JMIR Res Protoc. 2020 Apr 7;9(4):e16664. doi: 10.2196/16664.
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a serious, often life-threatening disease. In new-onset disease or a relapse, the standard treatment is immunosuppressive therapy with glucocorticoids; these therapies are associated with substantial short- and long-term toxicity. Complement component 5a (C5a) binding to C5a receptor (C5aR) may play a central role in the pathogenesis of ANCA-associated vasculitis. Avacopan is a novel, orally bioavailable, and highly selective antagonist of human C5aR. Avacopan does not interfere with the production of C5b or the membrane attack complex (ie, terminal complement complex) and does not block C5a binding to a second receptor, C5L2 (also called C5aR2), shown to be protective in antimyeloperoxidase glomerulonephritis. This trial will evaluate if avacopan replaces the need for chronic glucocorticoids in the treatment of ANCA-associated vasculitis.
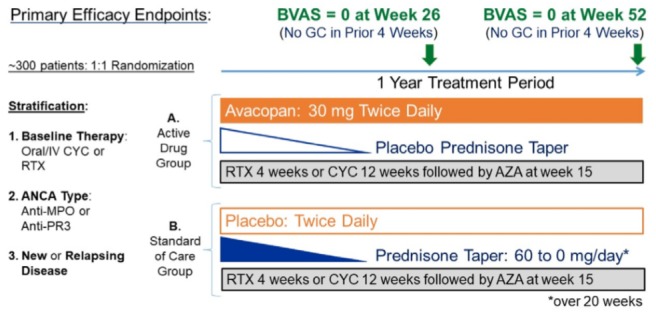
The aim of this study is to determine the proportions of patients in remission at week 26 and with sustained remission at week 52, defined as Birmingham Vasculitis Activity Score=0, and not taking glucocorticoids within the 4 weeks before week 26 and week 52, respectively.
The Avacopan Development in Vasculitis to Obtain Corticosteroid elimination and Therapeutic Efficacy study is a randomized, double-blind, active-comparator (prednisone), 2-arm study evaluating the safety and efficacy of avacopan versus prednisone, administered in combination with other immunosuppressive therapy. Eligible subjects will have active disease requiring induction of remission. Subjects are stratified based on the type of immunosuppressive therapy, ANCA subtype, and new or relapsing disease. Target sample size is 300 patients, enrolled at over 200 sites globally. All authors and local ethics committees approved the study design. All patients will provide informed consent.
Enrollment of patients was completed in Q4 2018. Topline results are anticipated to be published by Q3 2020.
Results will be released irrespective of whether the findings are positive or negative.
ClinicalTrials.gov NCT02994927; https://clinicaltrials.gov/ct2/show/NCT02994927.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/16664.
抗中性粒细胞胞浆抗体(ANCA)相关血管炎是一种严重的、常危及生命的疾病。在新发疾病或复发时,标准治疗是使用糖皮质激素进行免疫抑制治疗;这些治疗会带来严重的短期和长期毒性。补体成分5a(C5a)与C5a受体(C5aR)结合可能在ANCA相关血管炎的发病机制中起核心作用。阿伐可泮是一种新型的、口服生物可利用的、高度选择性的人C5aR拮抗剂。阿伐可泮不干扰C5b或膜攻击复合物(即末端补体复合物)的产生,也不阻断C5a与另一种受体C5L2(也称为C5aR2)的结合,C5L2在抗髓过氧化物酶肾小球肾炎中具有保护作用。本试验将评估阿伐可泮在治疗ANCA相关血管炎时是否可替代长期使用糖皮质激素的需求。
本研究的目的是确定在第26周达到缓解且在第52周持续缓解的患者比例,缓解定义为伯明翰血管炎活动评分=0,且在第26周和第52周前4周内未服用糖皮质激素。
阿伐可泮在血管炎中实现糖皮质激素消除和治疗效果的研究是一项随机、双盲、活性对照(泼尼松)、双臂研究,评估阿伐可泮与泼尼松联合其他免疫抑制治疗的安全性和有效性。符合条件的受试者将患有需要诱导缓解的活动性疾病。受试者根据免疫抑制治疗类型、ANCA亚型以及新发或复发疾病进行分层。目标样本量为300名患者,在全球200多个地点招募。所有作者和当地伦理委员会均批准了研究设计。所有患者均将提供知情同意书。
患者招募于2018年第四季度完成。预计在2020年第三季度公布初步结果。
无论结果是阳性还是阴性都将公布。
ClinicalTrials.gov NCT02994927;https://clinicaltrials.gov/ct2/show/NCT02994927。
国际注册报告识别码(IRRID):DERR1-10.2196/16664。