Department of Spine Surgery, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine for Nanjing University of Chinese Medicine, Nanjing 210028, Jiangsu, China.
Department of Anatomy, School of Basic Medical Sciences of Southwest Medical University, Luzhou 646000, Sichuan, China.
Biomed Res Int. 2020 Feb 7;2020:2960642. doi: 10.1155/2020/2960642. eCollection 2020.
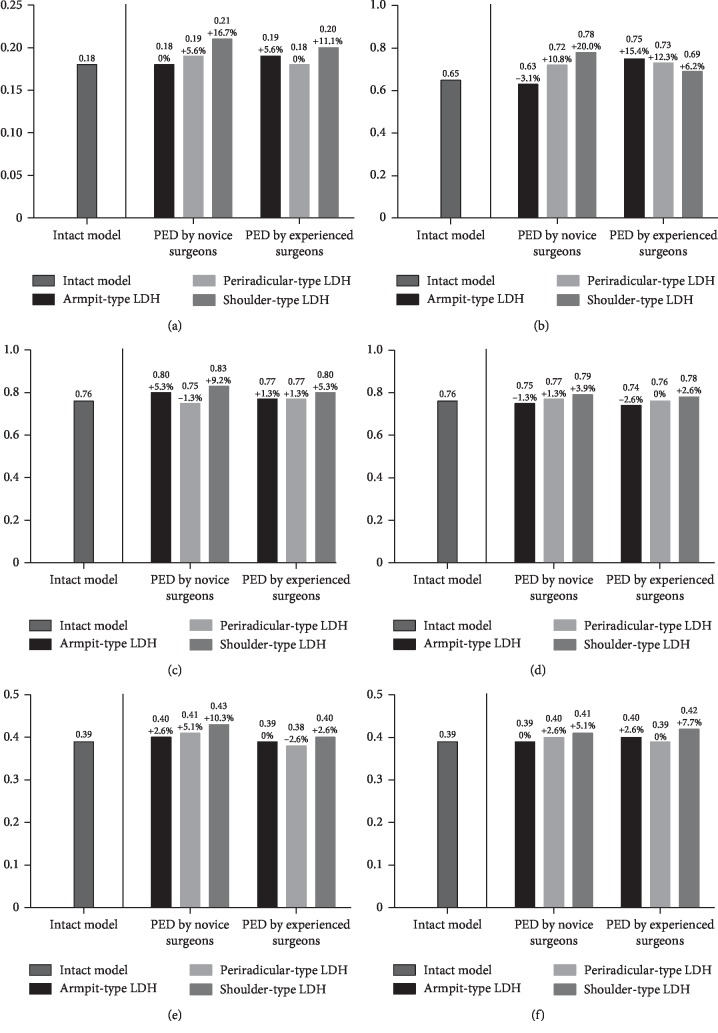
Translaminar percutaneous endoscopic discectomy (PED) was used widely in the treatment of lumbar disc herniation (LDH), especially for the training of novice surgeons. A larger range of osteotomy was a suitable method to get enough operation space and reduce intraoperative risks. But osteotomy, especially facetectomy, may be associated with the biomechanical deterioration and resulting adjacent segment diseases (ASD). Hence, the objects of this study were to investigate whether different levels of surgical experience in performing different ranges of osteotomy (especially facetectomy) affected the risk for ASD and to identify the safe indications for the training of PED novice surgeons. . In this study, a three-dimensional lumbosacral model was constructed and validated. Corresponding translaminar PED models with different ranges of osteotomy for armpit, periradicular, and shoulder types of LDH were constructed. The von Mises stress on the endplates, the shear stress on the annulus, the intradiscal pressure, and the range of motion (ROM) in the L3-L4 segment disc were computed.
Computational results in our well-validated model indicated that large ranges of osteotomy led to deterioration in most of the biomechanical indicators, and this trend was most significant in the shoulder-type LDH model.
To ensure the appropriateness of the surgical prognosis, armpit and periradicular types of LDH can be seen as suitable indications for the training of novice PED surgeons, and shoulder-type LDH should be excluded from such indications until novices can perform PED within a relatively small range of osteotomy. . Based on biomechanical variations in our finite element analysis, armpit and periradicular types of LDH can be seen as suitable indications for the training of novice PED surgeons, and shoulder-type LDH should be excluded until novices can perform PED within a relatively small range of osteotomy.
经皮内镜下腰椎间盘切除术(PED)广泛应用于腰椎间盘突出症(LDH)的治疗,尤其是对新手外科医生的培训。较大范围的截骨术是获得足够手术空间和降低术中风险的合适方法。但是截骨术,特别是关节突切除术,可能与生物力学恶化和由此导致的相邻节段疾病(ASD)有关。因此,本研究的目的是探讨不同经验水平的外科医生在进行不同范围截骨术(特别是关节突切除术)时,是否会增加 ASD 的风险,并确定 PED 新手外科医生培训的安全适应证。
在这项研究中,构建并验证了一个三维腰骶模型。构建了不同范围截骨术(腋窝型、神经根周围型和肩部型)的相应经皮内镜下腰椎间盘切除术模型。计算了终板上的 von Mises 应力、环上的剪切应力、椎间盘内压和 L3-L4 节段椎间盘的活动范围(ROM)。
计算结果表明,大范围截骨术会导致大多数生物力学指标恶化,这种趋势在肩部型 LDH 模型中最为明显。
为了确保手术预后的适当性,可以将腋窝型和神经根周围型 LDH 视为新手 PED 外科医生培训的合适适应证,而肩部型 LDH 应排除在这些适应证之外,直到新手能够在相对较小的截骨范围内进行 PED。基于我们有限元分析中的生物力学变化,可以将腋窝型和神经根周围型 LDH 视为新手 PED 外科医生培训的合适适应证,而肩部型 LDH 应排除在外,直到新手能够在相对较小的截骨范围内进行 PED。