Emerg Infect Dis. 2020 Mar;26(3):401-408. doi: 10.3201/eid2603.190571.
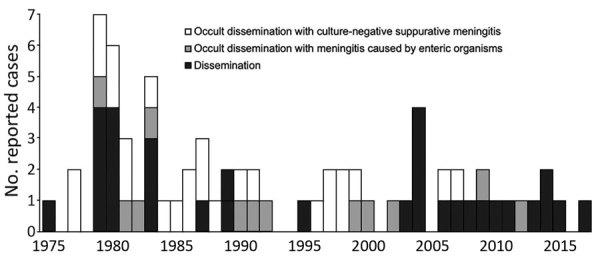
Clinical characteristics of disseminated strongyloidiasis, the severest form of strongyloidiasis, are not well described. We conducted a retrospective, consecutive chart review of patients with disseminated strongyloidiasis admitted to Okinawa Chubu Hospital in Okinawa, Japan, during January 1975-December 2017. The 70 patients were classified into 3 clinical phenotypes: dissemination (32 patients [45.7%]), occult dissemination with meningitis caused by enteric organisms (12 patients [17.1%]), and occult dissemination with culture-negative suppurative meningitis (26 patients [37.1%]). Associated mortality rates were 56.3%, 16.7%, and 11.5%, respectively, and sepsis occurred in 40.6%, 58.3%, and 11.5% of cases, respectively. Common symptoms included fever (52.9% of patients), headache (32.9%), and altered mental status (24.3%). Patients were treated with thiabendazole (before 2003) or ivermectin (after 2003). Our findings show that disseminated strongyloidiasis has clinical phenotypes in terms of severity and that identification of occult dissemination, a mild form with prominent neurologic manifestations, is lifesaving.
播散性粪类圆线虫病的临床特征(粪类圆线虫病最严重的形式)描述得并不清楚。我们对 1975 年 1 月至 2017 年 12 月期间在日本冲绳中部医院住院的播散性粪类圆线虫病患者进行了回顾性连续病历回顾。70 例患者分为 3 种临床表型:播散型(32 例[45.7%])、伴有肠道病原体引起的脑膜炎的隐匿性播散型(12 例[17.1%])和伴有Culture-negative 化脓性脑膜炎的隐匿性播散型(26 例[37.1%])。分别有 56.3%、16.7%和 11.5%的患者出现相关死亡率,分别有 40.6%、58.3%和 11.5%的患者发生脓毒症。常见症状包括发热(52.9%的患者)、头痛(32.9%)和精神状态改变(24.3%)。患者接受噻苯达唑(2003 年之前)或伊维菌素(2003 年之后)治疗。我们的研究结果表明,播散性粪类圆线虫病在严重程度方面存在临床表型,并且隐匿性播散型(一种以突出神经表现为特征的轻度形式)的识别具有挽救生命的意义。