Gottstein Bruno, Lachenmayer Anja, Beldi Guido, Wang Junhua, Merkle Bernadette, Vu Xuan Lan, Kurath Ursula, Müller Norbert
Institute of Parasitology, Department of Infectious Diseases and Pathobiology, Vetsuisse Faculty, University of Bern, Bern, Switzerland.
Institute for Infectious Diseases, Medical Faculty, University of Bern, Bern, Switzerland.
Food Waterborne Parasitol. 2019 May 8;16:e00055. doi: 10.1016/j.fawpar.2019.e00055. eCollection 2019 Sep.
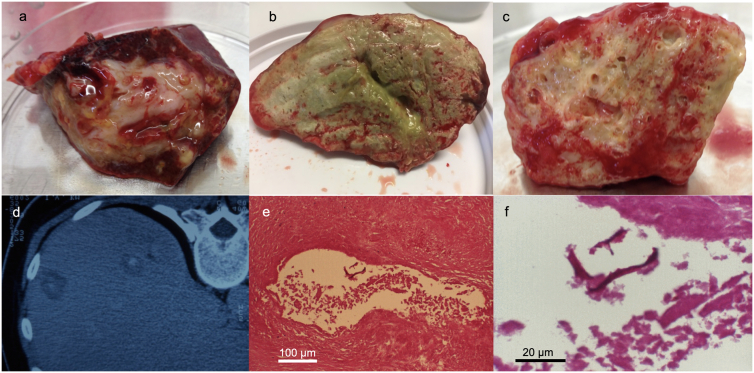
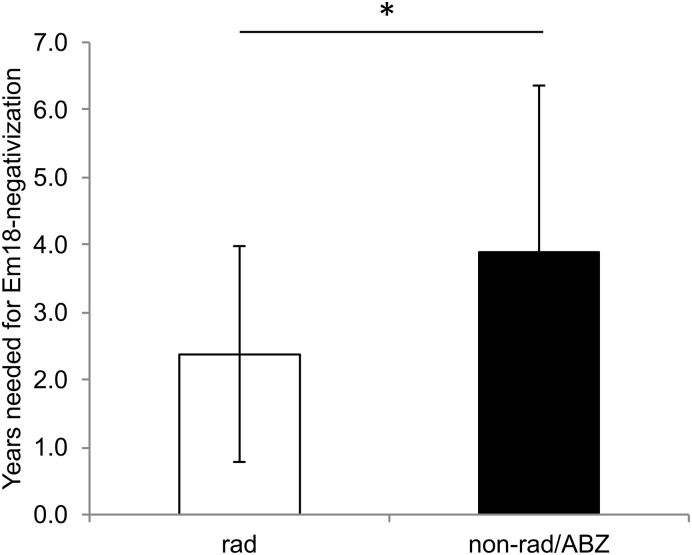
Diagnosis of alveolar echinococcosis (AE) is predominantly based on imaging procedures combined with immunodiagnostic testing. In the present study, we retrospectively analyzed the performance of four serological tests (EgHF-ELISA, Em2-ELISA, recEm18-ELISA and Em-Immunoblotting) for initial diagnosis and subsequent monitoring of AE patients. Overall, 101 AE patients were included, grouped according to treatment options and immune status as follows: (A) curative surgical treatment (n = 45 patients), (B) non-radical or palliative surgical treatment (n = 11), (C) benzimidazoles only (n = 20), (D) immunocompromised with radical surgical treatment (n = 11), (E) immunocompromised with benzimidazoles only (n = 4), and finally a group of 10 AE patients (F) that were considered to present so-called "abortive" lesions. Initial (i.e. pretreatment) ELISA-based diagnosis for patients in groups A to E revealed overall diagnostic sensitivities of 95% for EgHF, 86% for Em2, and 80% for recEm18, respectively. Comparatively, the diagnostic sensitivity of Em-Immunoblotting was higher with an overall value of 98%. In group F, only Em-Immunoblotting had an excellent diagnostic sensitivity (100%), whereas the ELISAs had poor sensitivities of 30% (EgHF- and Em2-ELISA) or even 0% (recEm18-ELISA). Serological monitoring of AE patients showed a clear association between a curative development of disease (induced either by surgery or benzimidazole medication) and a negativization in the ELISAs. This effect was most pronounced for the recEm18-ELISA, where 56% negativized following diagnosis/treatment, as compared to 36% for the EgHF-ELISA, and 37% for the Em2-ELISA, respectively. After radical surgery, the mean time until negativization in the recEm18-ELISA was 2.4 years (SD 1.6). This was significantly shorter than the mean 3.9 years (SD 2.5) in those AE patients with non-radical, palliative surgery or ABZ treatment who were able to negativize during the study period ( = 0.048). Conclusively, Em-Immunoblotting appears as the most sensitive test to diagnose active as well as inactive ("abortive") AE-cases. The inclusion of the ELISAs completes the initial diagnostic picture and offers valuable additional information. Conversely, recEm18-ELISA appears as the currently best serological tool to monitor a regressive and putatively curative course of AE in treated patients.
泡型包虫病(AE)的诊断主要基于影像学检查并结合免疫诊断检测。在本研究中,我们回顾性分析了四种血清学检测方法(EgHF-ELISA、Em2-ELISA、recEm18-ELISA和Em免疫印迹法)在AE患者初始诊断及后续监测中的表现。总共纳入了101例AE患者,根据治疗方案和免疫状态分为以下几组:(A)根治性手术治疗组(n = 45例患者),(B)非根治性或姑息性手术治疗组(n = 11例),(C)仅使用苯并咪唑组(n = 20例),(D)接受根治性手术治疗的免疫功能低下组(n = 11例),(E)仅使用苯并咪唑的免疫功能低下组(n = 4例),最后是一组10例被认为呈现所谓“顿挫型”病变的AE患者(F组)。对A至E组患者的初始(即治疗前)基于ELISA的诊断显示,EgHF的总体诊断敏感性为95%,Em2为86%,recEm18为80%。相比之下,Em免疫印迹法的诊断敏感性更高,总体值为98%。在F组中,只有Em免疫印迹法具有出色的诊断敏感性(100%),而ELISA的敏感性较差,EgHF-ELISA和Em2-ELISA为30%,recEm18-ELISA甚至为0%。AE患者的血清学监测显示,疾病的治愈性发展(由手术或苯并咪唑药物诱导)与ELISA结果转阴之间存在明显关联。这种效应在recEm18-ELISA中最为明显,诊断/治疗后56%的患者转阴,相比之下,EgHF-ELISA为36%,Em2-ELISA为37%。根治性手术后,recEm18-ELISA转阴的平均时间为2.4年(标准差1.6)。这明显短于在研究期间能够转阴的接受非根治性、姑息性手术或阿苯达唑治疗的AE患者的平均3.9年(标准差2.5)(P = 0.048)。总之,Em免疫印迹法似乎是诊断活动性和非活动性(“顿挫型”)AE病例最敏感的检测方法。ELISA的纳入完善了初始诊断情况并提供了有价值的额外信息。相反,recEm18-ELISA似乎是目前监测接受治疗患者中AE的消退和可能治愈过程的最佳血清学工具。