Department of Tumor Biology, Oslo University Hospital, Oslo, Norway.
Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
Cancer Biol Ther. 2020 May 3;21(5):432-440. doi: 10.1080/15384047.2020.1721252. Epub 2020 Feb 26.
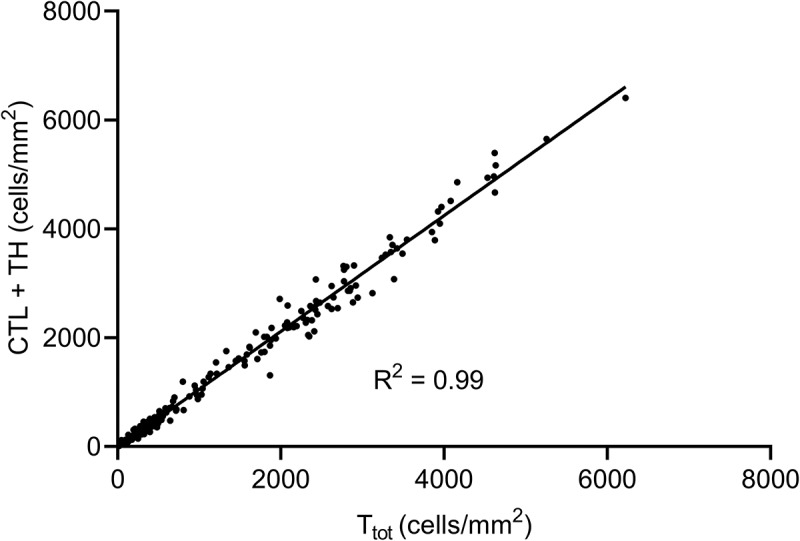
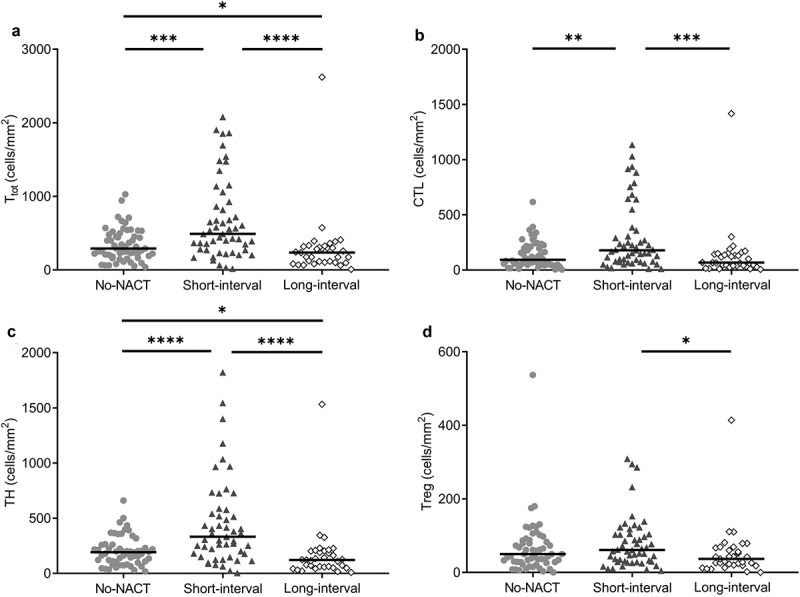
Patients with colorectal liver metastases (CLM) commonly receive neoadjuvant chemotherapy (NACT) prior to surgical resection. NACT may induce immunogenic cell death with subsequent recruitment of T-cells to the tumor microenvironment, which could be exploited by immune checkpoint inhibition (ICI). In theory, this could expand the use of ICI to obtain responses also in microsatellite stable colorectal cancer, but evidence to suggest optimal treatment schedules are lacking. In this study, densities of total-, cytotoxic-, helper- and regulatory T-cells were quantified by immunohistochemistry in resected CLM from 92 patients included in the OSLO-COMET trial (NCT01516710). All but one patient had microsatellite stable tumors (91/92). Associations between T-cell densities and clinicopathological parameters were analyzed. Fluoropyrimidine-based NACT (in most cases with addition of oxaliplatin or irinotecan) was administered to 45 patients completed median 8 weeks prior to surgical resection. No overall association was found between NACT administration and intratumoral T-cell densities. However, within the NACT group, a short time interval (<9.5 weeks) between NACT completion and CLM resection was strongly associated with high intratumoral T-cell densities compared to the long-interval and no NACT groups (medians 491, 236, and 292 cells/mm, respectively; < .0001). The results from this study suggest that the observed increase in intratumoral T-cells after NACT administration may be transient. The significance of this finding should be further explored to ensure that optimal treatment schedules are chosen for studies combining cytotoxic chemotherapy and ICI.
结直肠癌肝转移(CLM)患者在手术切除前通常接受新辅助化疗(NACT)。NACT 可能诱导免疫原性细胞死亡,随后招募 T 细胞进入肿瘤微环境,这可以被免疫检查点抑制(ICI)利用。从理论上讲,这可以扩大 ICI 的使用范围,使微卫星稳定的结直肠癌也能获得应答,但缺乏表明最佳治疗方案的证据。在这项研究中,通过免疫组化定量分析了 OSLO-COMET 试验(NCT01516710)中 92 例接受手术切除的 CLM 患者的总 T 细胞、细胞毒性 T 细胞、辅助 T 细胞和调节性 T 细胞的密度。除 1 例患者外,所有患者的肿瘤均为微卫星稳定型(91/92)。分析了 T 细胞密度与临床病理参数之间的关系。45 例患者接受了氟嘧啶类 NACT(大多数情况下加用奥沙利铂或伊立替康),中位时间为 8 周,然后进行手术切除。未发现 NACT 给药与肿瘤内 T 细胞密度之间存在总体相关性。然而,在 NACT 组中,NACT 完成与 CLM 切除之间的时间间隔较短(<9.5 周)与高肿瘤内 T 细胞密度强烈相关,与长间隔和无 NACT 组相比(中位数分别为 491、236 和 292 个细胞/mm;<0.0001)。这项研究的结果表明,NACT 给药后观察到的肿瘤内 T 细胞增加可能是短暂的。应进一步探讨这一发现的意义,以确保为联合细胞毒性化疗和 ICI 的研究选择最佳治疗方案。