Division of Cardiovascular Sciences, Cardiac Centre, Faculty of Medical and Human Sciences, University of Manchester and NIHR/Wellcome Trust Clinical Research Facility, Manchester, UK.
Cardiovascular Trials Unit, Central Manchester University Hospital NHS Foundation Trust, Manchester, UK.
Sci Rep. 2020 Feb 25;10(1):3371. doi: 10.1038/s41598-020-60422-7.
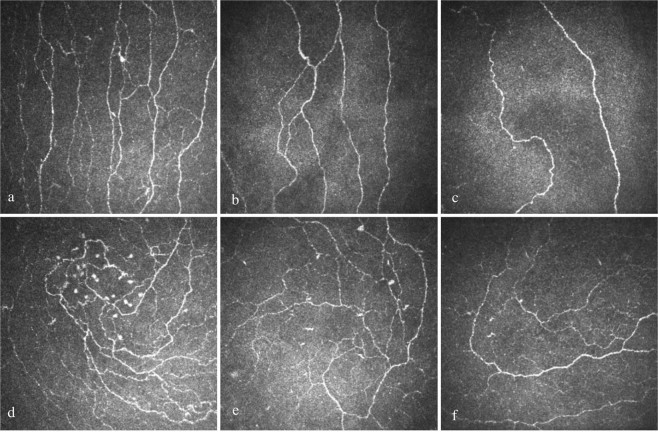
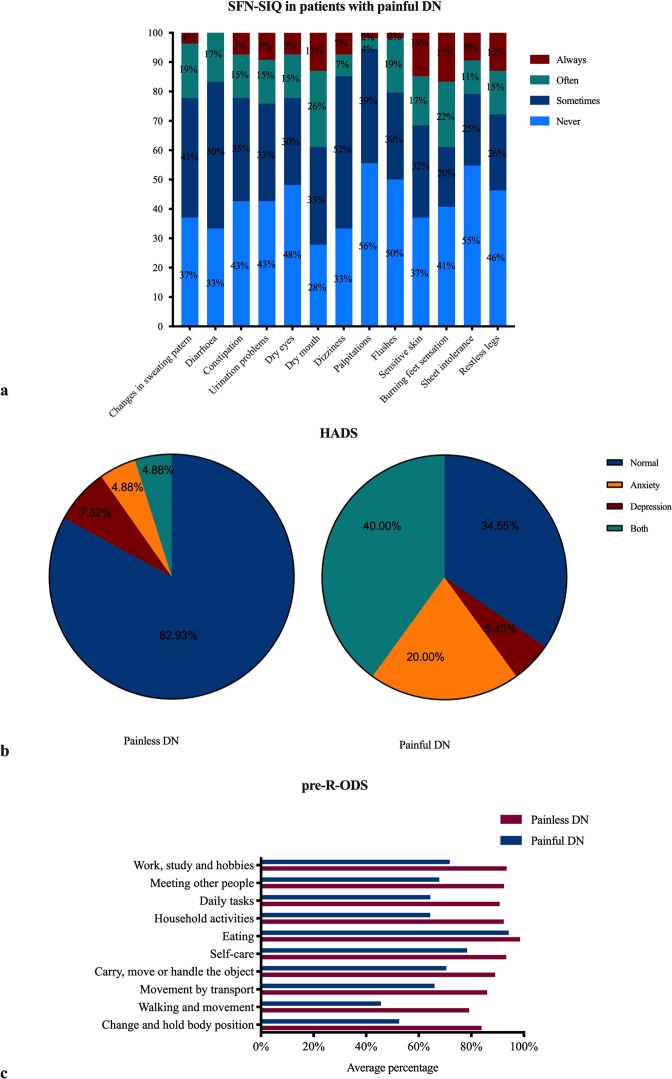
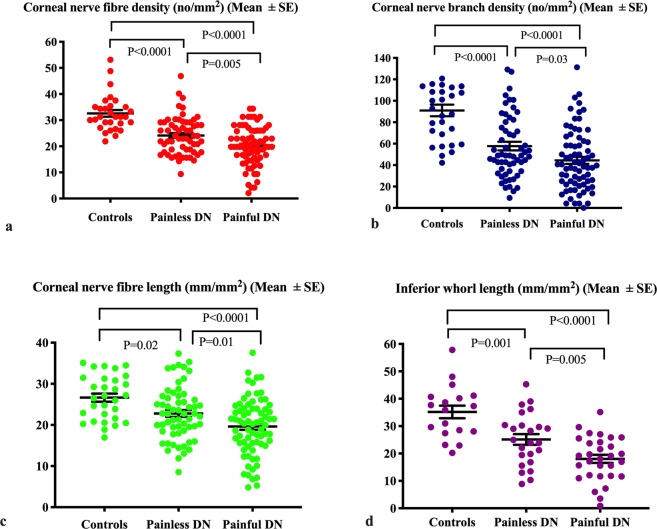
Neuropathic pain is believed to arise from damage to nociceptive C fibres in diabetic neuropathy (DN). We have utilised corneal confocal microscopy (CCM) to quantify the severity of small nerve fibre damage in relation to the severity of neuropathic pain and quality of life (QoL) in patients with and without painful DN. 30 controls and patients with painful (n = 78) and painless (n = 62) DN underwent assessment of large and small nerve fibre function, CCM, neuropathic symptoms (small fibre neuropathy symptom inventory questionnaire, neuropathic pain scale) and QoL (SF-36, pre-R-ODS and hospital anxiety and depression scale). Patients with painful compared to painless DN, had comparable neurophysiology and vibration perception, but lower corneal nerve fibre density (20.1 ± 0.87 vs. 24.13 ± 0.91, P = 0.005), branch density (44.4 ± 3.31 vs. 57.74 ± 3.98, P = 0.03), length (19.61 ± 0.81 vs. 22.77 ± 0.83, P = 0.01), inferior whorl length (18.03 ± 1.46 vs. 25.1 ± 1.95, P = 0.005) and cold sensation threshold (21.35 ± 0.99 vs. 26.08 ± 0.5, P < 0.0001) and higher warm sensation threshold (43.7 ± 0.49 vs. 41.37 ± 0.51, P = 0.004) indicative of small fibre damage. There was a significant association between all CCM parameters and the severity of painful neuropathic symptoms, depression score and QoL. CCM identifies small nerve fibre loss, which correlates with the severity of neuropathic symptoms and reduced QoL in patients with painful diabetic neuropathy.
神经病理性疼痛被认为源于糖尿病性周围神经病(DN)中伤害感受 C 纤维的损伤。我们利用角膜共聚焦显微镜(CCM)来量化小纤维损伤的严重程度与有或无疼痛性 DN 的患者的神经病理性疼痛严重程度和生活质量(QoL)之间的关系。30 名对照者和有疼痛性(n=78)和无痛性(n=62)DN 的患者接受了大纤维和小纤维功能、CCM、神经病理性症状(小纤维神经病症状量表问卷、神经病理性疼痛量表)和 QoL(SF-36、预 R-ODS 和医院焦虑和抑郁量表)评估。与无痛性 DN 相比,疼痛性 DN 的患者具有可比的神经生理学和振动感觉,但角膜神经纤维密度更低(20.1±0.87 对 24.13±0.91,P=0.005)、分支密度更低(44.4±3.31 对 57.74±3.98,P=0.03)、长度更短(19.61±0.81 对 22.77±0.83,P=0.01)、下涡旋长度更短(18.03±1.46 对 25.1±1.95,P=0.005)和冷感觉阈值更高(21.35±0.99 对 26.08±0.5,P<0.0001)以及温觉阈值更高(43.7±0.49 对 41.37±0.51,P=0.004),提示小纤维损伤。所有 CCM 参数与疼痛性神经病理性症状的严重程度、抑郁评分和 QoL 之间均存在显著相关性。CCM 可识别小神经纤维的丧失,这与疼痛性糖尿病性周围神经病患者的神经病理性症状严重程度和 QoL 降低相关。