Ho Vivian, Tapaneeyakul Sasathorn, Metcalfe Leanne, Vu Lan, Short Marah
Baker Institute for Public Policy, Rice University, 6100 Main Street, MS 22, Houston, TX 77005, USA.
Department of Economics, Rice University, Houston, TX, USA.
Health Serv Outcomes Res Methodol. 2020 Mar;20(1):1-12. doi: 10.1007/s10742-020-00207-7. Epub 2020 Feb 4.
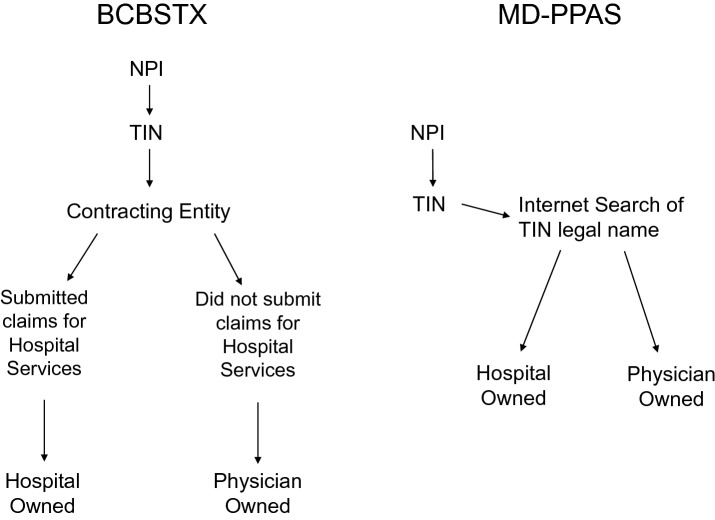
Researchers, healthcare providers, and policy makers have become increasingly interested in the cost and quality effects of vertical integration (VI) between hospitals and physicians. However, tracking VI is often financially costly. Because the Medicare Data on Provider Practice and Specialty (MD-PPAS) annual dataset may be more cost-effective for researchers to access than private data sources, we examine the accuracy of MD-PPAS in identifying VI by comparing it to physician and hospital affiliations reported in Blue Cross Blue Shield Texas (BCBSTX) PPO claims data for 2014-2016. The BCBSTX data serve as a gold standard, because physician-hospital affiliations are based on the insurer's provider contract information. We merged the two datasets using the physician National Provider Identifier (NPI), then determined what percentage of physicians had the same Tax Identification Number (TIN) in both sources, and whether the TIN implied the physician belonged to a physician- or hospital-owned practice. We found that 71.3% of successfully matched NPIs reported the same TIN, and 95.1% of patient-level observations were attributed to organizations with the same ownership type in both datasets, regardless of TIN. We compared regression estimates of patient-level annual spending on an indicator variable for physician versus hospital ownership for the primary attributed physician and found that estimates were within one percentage point whether one determined VI based on the BCBSTX or the MD-PPAS data. The results suggest that MD-PPAS, which costs less to obtain than from a for-profit data source, can be used to reliably track VI between hospitals and physicians.
研究人员、医疗服务提供者和政策制定者对医院与医生之间纵向整合(VI)的成本和质量影响越来越感兴趣。然而,追踪纵向整合在财务上往往成本高昂。由于医疗保险提供者执业与专业数据(MD-PPAS)年度数据集对研究人员来说可能比私人数据源更具成本效益,我们通过将其与2014 - 2016年蓝十字蓝盾德克萨斯州(BCBSTX)优先提供者组织(PPO)索赔数据中报告的医生和医院附属关系进行比较,来检验MD-PPAS在识别纵向整合方面的准确性。BCBSTX数据作为黄金标准,因为医生与医院的附属关系基于保险公司的提供者合同信息。我们使用医生国家提供者识别码(NPI)合并了这两个数据集,然后确定在两个数据源中具有相同税务识别号(TIN)的医生百分比,以及该TIN是否意味着医生属于医生所有或医院所有的执业机构。我们发现,71.3%成功匹配的NPI报告了相同的TIN,并且95.1%的患者层面观察结果归因于两个数据集中具有相同所有权类型的组织,无论TIN如何。我们比较了针对主要归因医生的患者层面年度支出关于医生与医院所有权指标变量的回归估计,发现无论基于BCBSTX还是MD-PPAS数据来确定纵向整合,估计值都在一个百分点以内。结果表明,获取成本低于营利性数据源的MD-PPAS可用于可靠地追踪医院与医生之间的纵向整合。