Department of Radiation Oncology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, No.138, Sheng Li Road, Tainan, 70456, Taiwan.
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Radiat Oncol. 2020 Feb 27;15(1):48. doi: 10.1186/s13014-020-01498-3.
The literature regarding pericardial effusion after definitive concurrent chemotherapy and intensity modulated radiotherapy (IMRT) for esophageal cancer was lacking. This study aimed to investigate the risk factors of pericardial effusion in esophageal cancer patients undergoing definitive concurrent chemotherapy and IMRT.
A total of 126 consecutive esophageal cancer patients treated with definitive concurrent chemotherapy and IMRT between 2008 and 2018 were reviewed. The pericardial effusion was determined on computed tomography scan of the chest and graded by the Common Terminology Criteria for Adverse Events, version 4.0. The cumulative incidence of pericardial effusion was estimated by the Kaplan-Meier method and compared between groups by the log-rank test. The risk factors of pericardial effusion were determined with multivariate Cox proportional hazards regression analysis.
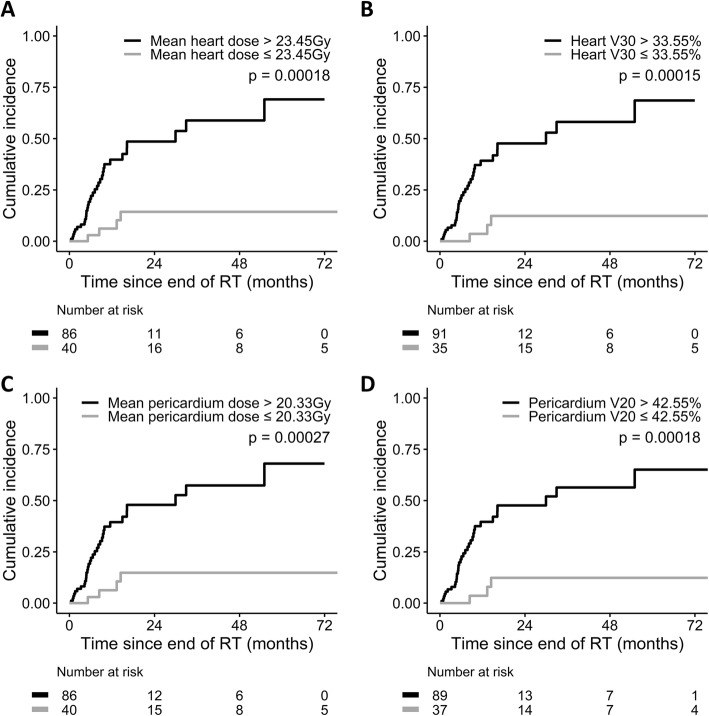
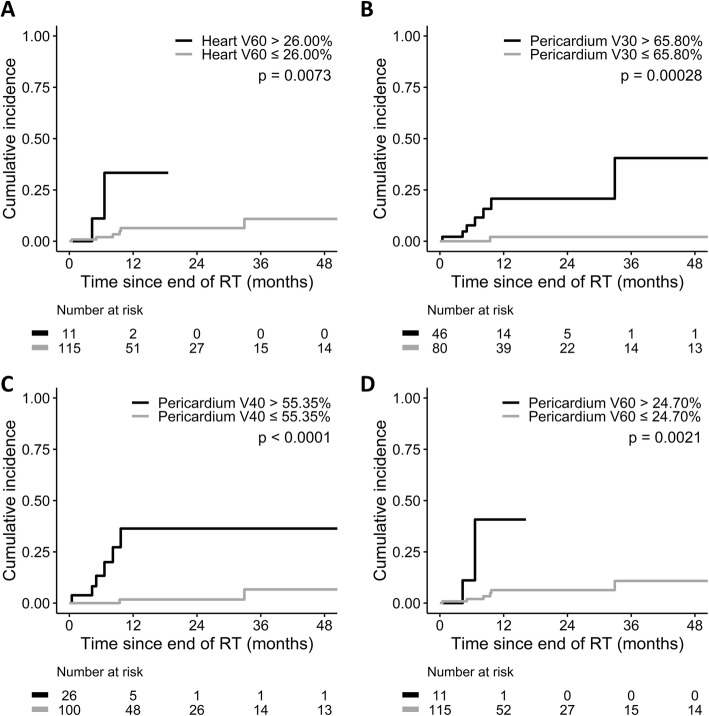
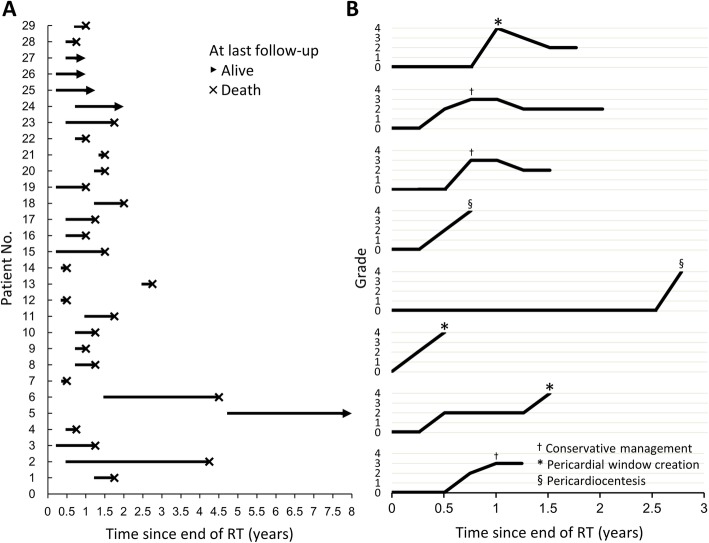
The median follow-up time was 14.0 months. Thirty-seven (29.4%) patients had pericardial effusion after a median interval of 6.6 months since the end of IMRT. The cumulative incidence of pericardial effusion of any grade was higher in patients with mean heart dose > 23.45 Gy (p = 0.00018), heart V30 > 33.55% (p = 0.00015), mean pericardium dose > 20.33 Gy (p = 0.00027), and pericardium V20 > 42.55% (p = 0.00018). Furthermore, eight (6.3%) patients had symptoms related to pericardial effusion and were considered as cases with pericardial effusion ≥ grade 3. The cumulative incidence of pericardial effusion ≥ grade 3 was higher in patients with pericardium V30 > 65.80% (p = 0.00028), V40 > 55.35% (p < 0.0001), and V60 > 24.70% (p = 0.0021). Multivariate analyses showed the above dose-volume parameters predicted the risk of pericardial effusion in esophageal cancer.
Dose-volume parameters predicting the risk of pericardial effusion were identified in esophageal cancer treated with definitive concurrent chemotherapy and IMRT. They could be applied as constraints of IMRT for esophageal cancer.
关于接受根治性同步化疗和调强放疗(IMRT)治疗食管癌后出现心包积液的文献资料较为缺乏。本研究旨在探讨接受根治性同步化疗和 IMRT 治疗的食管癌患者发生心包积液的危险因素。
回顾性分析 2008 年至 2018 年期间接受根治性同步化疗和 IMRT 治疗的 126 例连续食管癌患者的临床资料。通过胸部计算机断层扫描确定心包积液,并根据通用不良事件术语标准 4.0 进行分级。采用 Kaplan-Meier 法估计心包积液的累积发生率,并采用对数秩检验比较各组之间的差异。采用多因素 Cox 比例风险回归分析确定心包积液的危险因素。
中位随访时间为 14.0 个月。37 例(29.4%)患者在 IMRT 结束后 6.6 个月时出现心包积液。中位心剂量>23.45 Gy(p=0.00018)、心脏 V30>33.55%(p=0.00015)、平均心包剂量>20.33 Gy(p=0.00027)和心包 V20>42.55%(p=0.00018)的患者心包积液任何分级的累积发生率更高。此外,8 例(6.3%)患者有心包积液相关症状,被认为是心包积液≥3 级的患者。心包 V30>65.80%(p=0.00028)、V40>55.35%(p<0.0001)和 V60>24.70%(p=0.0021)的患者心包积液≥3 级的累积发生率更高。多因素分析表明,上述剂量-体积参数可预测食管癌患者心包积液的风险。
本研究确定了接受根治性同步化疗和 IMRT 治疗的食管癌患者发生心包积液的风险预测剂量-体积参数。这些参数可作为食管癌调强放疗的限制条件。