Department of Radiation Oncology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
PLoS One. 2020 Aug 6;15(8):e0237114. doi: 10.1371/journal.pone.0237114. eCollection 2020.
This study aimed to investigate the correlation between primary tumor volume and cancer failure patterns in esophageal squamous cell carcinoma (ESCC) treated with definitive concurrent chemoradiotherapy (CCRT) and examine whether increasing radiation dose can improve the outcome.
We retrospectively reviewed 124 patients with stage III ESCC treated by definitive CCRT. The primary tumor volume calculated from the radiotherapy planning computed tomography scans was correlated to treatment response, time to disease progression, and overall survival. We further analyzed whether a higher radiation dose correlated with better disease control and patient survival.
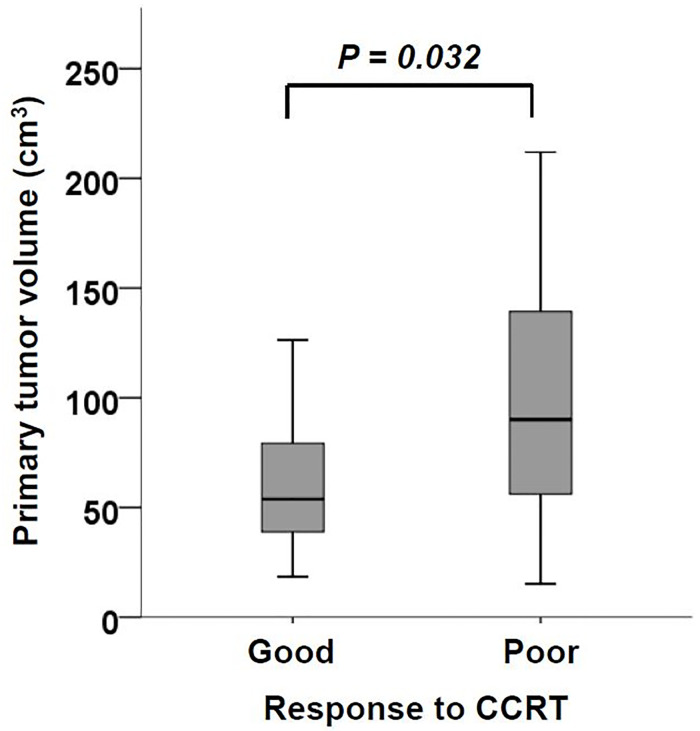
Patients with poor CCRT response had a larger primary tumor volume than those with good response (97.9 vs 64.3 cm3, P = 0.032). The optimal cutoff value to predict CCRT response was 55.3 cm3. Large primary tumor volume (≥ 55.3 cm3) correlated with shorter time to tumor progression in the esophagus (13.6 vs 48.6 months, P = 0.033) compared with small tumor volume (< 55.3 cm3). For the large esophageal tumors (≥ 55.3 cm3), radiation dose > 60 gray significantly prolonged the time to tumor progression in esophagus (20.3 vs 10.1 months, P = 0.036) and overall survival (12.2 vs 8.0 months, P = 0.030), compared with dose ≤ 60 gray. In contrast, higher radiation dose did not benefit local disease control or overall survival in the small esophageal tumors (< 55.3 cm3).
Large primary tumor volume correlates with poor local control and overall survival in ESCC treated with definitive CCRT. Radiation dose > 60 gray can improve the outcomes in patients with large primary tumor. Further prospective dose escalation trials are warranted.
本研究旨在探讨经根治性同步放化疗(CCRT)治疗的食管鳞癌(ESCC)中原发肿瘤体积与癌症失败模式的相关性,并研究增加放疗剂量是否能改善预后。
我们回顾性分析了 124 例接受根治性 CCRT 治疗的 III 期 ESCC 患者。从放疗计划 CT 扫描中计算出的原发肿瘤体积与治疗反应、疾病进展时间和总生存时间相关。我们进一步分析了更高的放疗剂量是否与更好的疾病控制和患者生存相关。
CRT 反应不佳的患者原发肿瘤体积大于反应良好的患者(97.9cm3 vs 64.3cm3,P = 0.032)。预测 CRT 反应的最佳截断值为 55.3cm3。与小肿瘤体积(<55.3cm3)相比,大原发肿瘤体积(≥55.3cm3)与食管肿瘤进展时间更短相关(13.6 个月 vs 48.6 个月,P = 0.033)。对于大食管肿瘤(≥55.3cm3),放疗剂量>60Gy 显著延长食管肿瘤进展时间(20.3 个月 vs 10.1 个月,P = 0.036)和总生存时间(12.2 个月 vs 8.0 个月,P = 0.030),与剂量≤60Gy 相比。相比之下,大原发肿瘤体积与小食管肿瘤(<55.3cm3)的局部疾病控制或总生存无显著相关性。
在接受根治性 CCRT 治疗的 ESCC 中,大原发肿瘤体积与局部控制不良和总生存时间相关。放疗剂量>60Gy 可以改善大原发肿瘤患者的预后。需要进一步开展前瞻性剂量递增试验。