Department of Liver Disease and Digestive Interventional Radiology, National Clinical Research Center for Digestive Diseases and Xijing Hospital of Digestive Diseases, Fourth Military Medical University, Xi'an 710032, Shaanxi Province, China.
Department of Radiology, the Southwest Hospital, Third Military Medical University, Chongqing 400037, China.
World J Gastroenterol. 2020 Feb 14;26(6):657-669. doi: 10.3748/wjg.v26.i6.657.
The treatment outcome of transarterial chemoembolization (TACE) in unresectable hepatocellular carcinoma (HCC) varies greatly due to the clinical heterogeneity of the patients. Therefore, several prognostic systems have been proposed for risk stratification and candidate identification for first TACE and repeated TACE (re-TACE).
To investigate the correlations between prognostic systems and radiological response, compare the predictive abilities, and integrate them in sequence for outcome prediction.
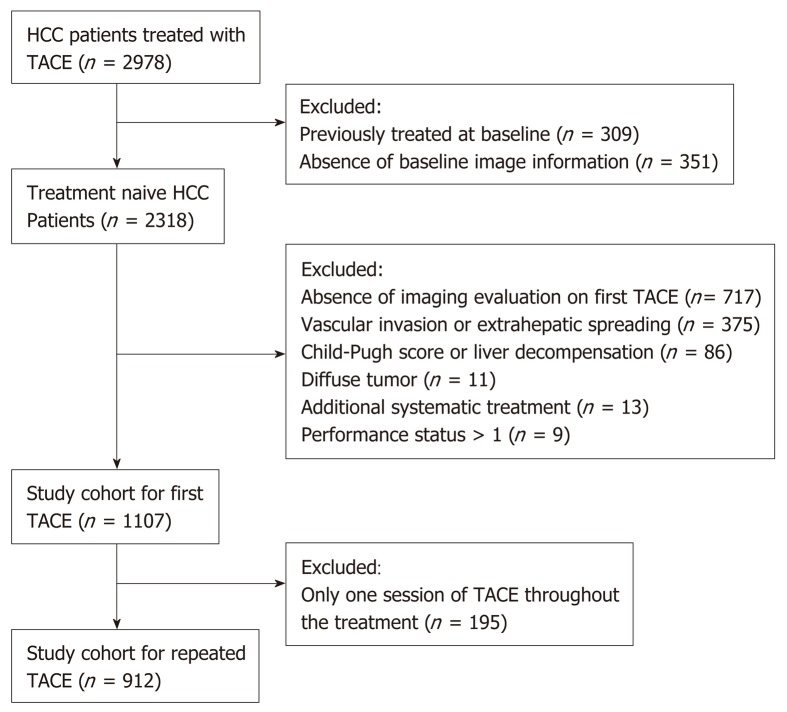
This nationwide multicenter retrospective cohort consisted of 1107 unresectable HCC patients in 15 Chinese tertiary hospitals from January 2010 to May 2016. The Hepatoma Arterial-embolization Prognostic (HAP) score system and its modified versions (mHAP, mHAP2 and mHAP3), as well as the six-and-twelve criteria were compared in terms of their correlations with radiological response and overall survival (OS) prediction for first TACE. The same analyses were conducted in 912 patients receiving re-TACE to evaluate the ART (assessment for re-treatment with TACE) and ABCR (alpha-fetoprotein, Barcelona Clinic Liver Cancer, Child-Pugh and Response) systems for post re-TACE survival (PRTS).
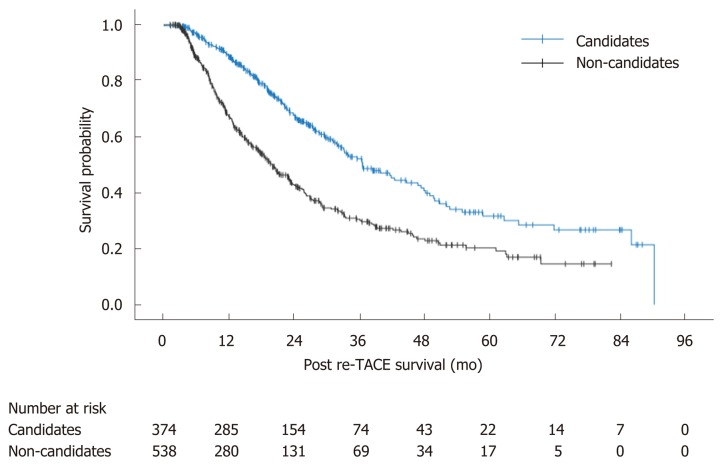
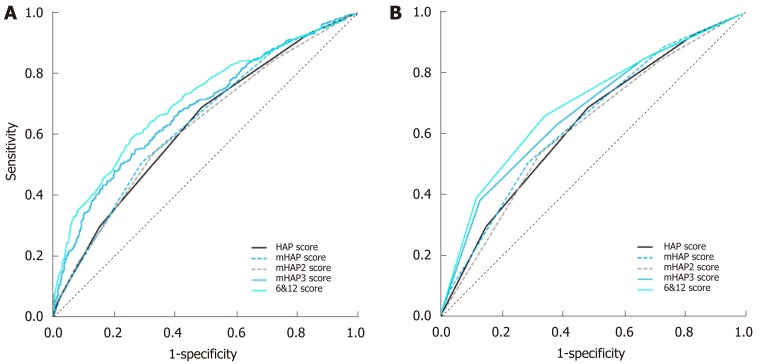
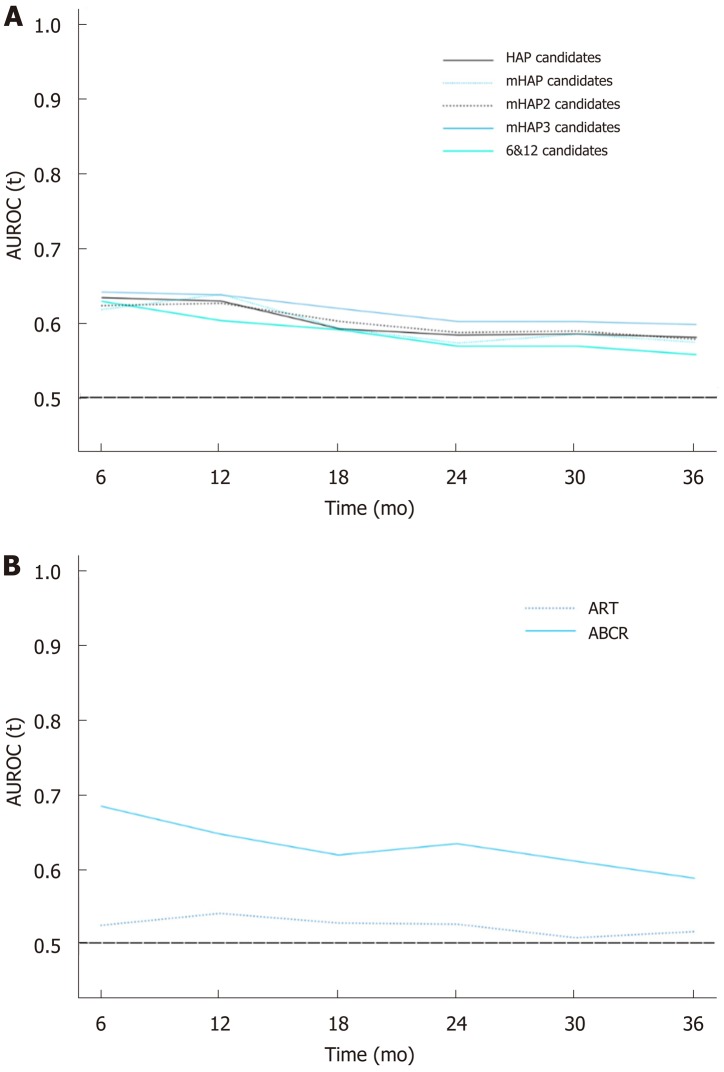
All the prognostic systems were correlated with radiological response achieved by first TACE, and the six-and-twelve criteria exhibited the highest correlation (Spearman R = 0.39, = 0.026) and consistency (Kappa = 0.14, = 0.019), with optimal performance by area under the receiver operating characteristic curve of 0.71 [95% confidence interval (CI): 0.68-0.74]. With regard to the prediction of OS, the mHAP3 system identified patients with a favorable outcome with the highest concordance (C)-index of 0.60 (95%CI: 0.57-0.62) and the best area under the receiver operating characteristic curve at any time point during follow-up; whereas, PRTS was well-predicted by the ABCR system with a C-index of 0.61 (95%CI: 0.59-0.63), rather than ART. Finally, combining the mHAP3 and ABCR systems identified candidates suitable for TACE with an improved median PRTS of 36.6 mo, compared with non-candidates with a median PRTS of 20.0 mo (log-rank test < 0.001).
Radiological response to TACE is closely associated with tumor burden, but superior prognostic prediction could be achieved with the combination of mHAP3 and ABCR in patients with unresectable liver-confined HCC.
由于患者的临床异质性,经动脉化疗栓塞术(TACE)治疗不可切除肝细胞癌(HCC)的治疗结果差异很大。因此,已经提出了几种预后系统,用于风险分层和候选识别,以进行首次 TACE 和重复 TACE(re-TACE)。
探讨预后系统与影像学反应之间的相关性,比较预测能力,并对其进行序列整合以进行结果预测。
本研究为全国性多中心回顾性队列研究,纳入了 2010 年 1 月至 2016 年 5 月期间来自中国 15 家三级医院的 1107 例不可切除 HCC 患者。比较了肝癌动脉栓塞预后(HAP)评分系统及其改良版(mHAP、mHAP2 和 mHAP3)以及六二标准与首次 TACE 的影像学反应和总生存(OS)预测的相关性。在接受 re-TACE 的 912 例患者中进行了相同的分析,以评估评估再治疗 TACE(ART)和 ABCR(alpha-fetoprotein,Barcelona Clinic Liver Cancer,Child-Pugh 和 Response)系统在 post re-TACE 生存(PRTS)中的作用。
所有预后系统均与首次 TACE 获得的影像学反应相关,六二标准显示出最高的相关性(Spearman R = 0.39, = 0.026)和一致性(Kappa = 0.14, = 0.019),其最佳表现为受试者工作特征曲线下面积为 0.71 [95%置信区间(CI):0.68-0.74]。在 OS 预测方面,mHAP3 系统具有最高的一致性(C)指数为 0.60(95%CI:0.57-0.62),并在随访期间的任何时间点都具有最佳的受试者工作特征曲线下面积,可识别出预后良好的患者;而 PRTS 则由 ABCR 系统很好地预测,其 C 指数为 0.61(95%CI:0.59-0.63),而非 ART。最后,结合 mHAP3 和 ABCR 系统,可以识别出适合 TACE 的候选者,其中位 PRTS 为 36.6 个月,而不适合候选者的中位 PRTS 为 20.0 个月(对数秩检验<0.001)。
TACE 的影像学反应与肿瘤负荷密切相关,但结合 mHAP3 和 ABCR 可以提高不可切除的肝局限性 HCC 患者的预后预测能力。