Yang Qing, Wang Ting, Ai Lei, Jiang Kai, Tao Xingguang, Gong Dongliang, Chen Nong, Fu Yang, Pan Fugen
Department of Orthopedics, QingPu Branch of Zhongshan Hospital Affiliated to Fudan University, Qingpu District Central Hospital of Shanghai, Shanghai 201700, P.R. China.
Department of Gastroenterology, Shanghai General Hospital, Shanghai Jiao Tong University, Shanghai 201600, P.R. China.
Exp Ther Med. 2020 Mar;19(3):2252-2258. doi: 10.3892/etm.2020.8445. Epub 2020 Jan 10.
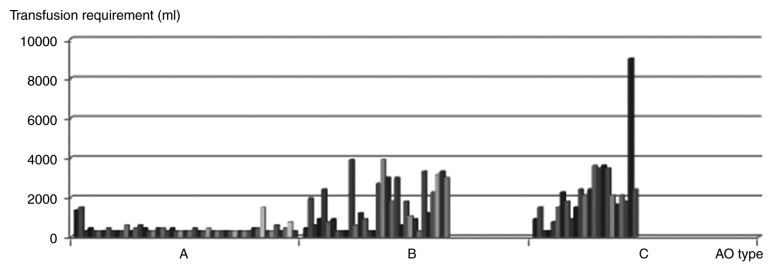
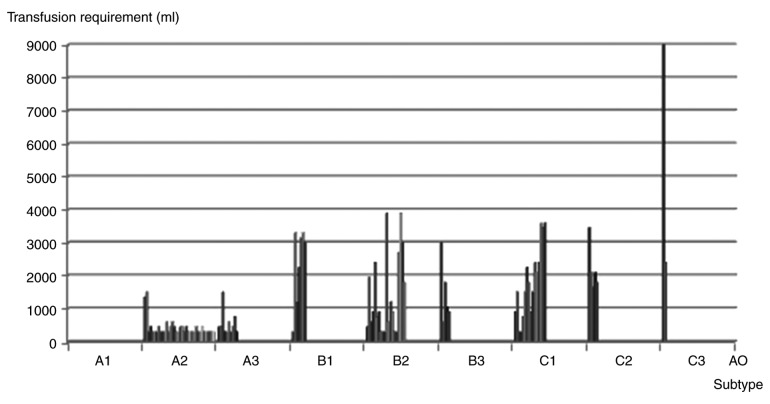
As part of the treatment of pelvic fracture, major hemorrhage poses a challenge for trauma surgeons. The aim of the present study was to evaluate the clinical outcomes of blood transfusion in the initial 6 h after pelvic fracture, and to define the blood transfusion volume required for each pelvic fracture type. A retrospective cohort study was performed on patients with pelvic fracture at a single Level I Trauma Centre over a 3-year period. A total of 1,297 patients were transported to our trauma centre within 2 h of injury and blood transfusion was administered in the initial 6 h after pelvic fracture. Review of the patients' medical records provided the initial pelvic radiographs and data from emergency department care. Clinical outcomes, including frequency of blood transfusion, blood transfusion volume, injury severity scores and mortality, were evaluated. All pelvic fractures were defined as closed fractures and patients were categorized according to the Arbeit fuer Osteosynthese (AO) classification system. Statistical methods were used to identify trends to provide guidance for clinical prediction. Complete data were available for 497 patients with pelvic fracture, 104 (20.9%) of which received blood transfusion. The blood transfusion volume in the initial 6 h ranged from 0 to 10,000 ml, with a mean of 1,213.94±1354.11 ml. The total mortality rate was 1.8%. Among the patients with C-type pelvic fractures, the frequency of blood transfusion was 59.0% and the mean volume was 2,191.30±1,740.93 ml. The mortality rate for C-type pelvic fractures was 11.43%. The B3 subtype of pelvic fractures had the highest transfusion frequency (53.6%), while the C3 subtype had the largest blood transfusion volume (5,700.00±4,666.90 ml). Patients with type A-C pelvic fractures had a progressively larger mean transfusion volume, transfusion frequency and mortality in the initial 6 h after pelvic fracture. The AO classification system was demonstrated to be a useful tool for the identification of pelvic fracture risk in the present study.
作为骨盆骨折治疗的一部分,严重出血给创伤外科医生带来了挑战。本研究的目的是评估骨盆骨折后最初6小时内输血的临床结果,并确定每种骨盆骨折类型所需的输血量。在一家一级创伤中心对骨盆骨折患者进行了为期3年的回顾性队列研究。共有1297例患者在受伤后2小时内被送往我们的创伤中心,并在骨盆骨折后的最初6小时内进行了输血。查阅患者的病历可获得最初的骨盆X光片和急诊科护理数据。评估了临床结果,包括输血频率、输血量、损伤严重程度评分和死亡率。所有骨盆骨折均定义为闭合性骨折,并根据瑞士内固定协会(AO)分类系统对患者进行分类。采用统计方法识别趋势,为临床预测提供指导。497例骨盆骨折患者获得了完整数据,其中104例(20.9%)接受了输血。最初6小时内的输血量为0至10000毫升,平均为1213.94±1354.11毫升。总死亡率为1.8%。在C型骨盆骨折患者中,输血频率为59.0%,平均输血量为2191.30±1740.93毫升。C型骨盆骨折的死亡率为11.43%。骨盆骨折的B3亚型输血频率最高(53.6%),而C3亚型输血量最大(5700.00±4666.90毫升)。A-C型骨盆骨折患者在骨盆骨折后最初6小时内的平均输血量、输血频率和死亡率逐渐增加。在本研究中,AO分类系统被证明是识别骨盆骨折风险的有用工具。