Sidebottom Abbey C, Vacquier Marc C, Jensen Joseph C, Bradley Steven M, Knickelbine Thomas, Strauss Craig, Miedema Michael D
Care Delivery Research, Allina Health, Minneapolis, Minnesota.
Minneapolis Heart Institute Foundation, Minneapolis, Minnesota.
Clin Cardiol. 2020 Jun;43(6):560-567. doi: 10.1002/clc.23347. Epub 2020 Feb 27.
The 2013 ACC/AHA (American College of Cardiology/American Heart Association) cholesterol guidelines provided an evidence-based rationale for the allocation of lipid-lowering therapy based on risk for atherosclerotic cardiovascular disease (ASCVD). Adoption of these guidelines was initially suboptimal but whether this has improved over time remains unclear.
Prevalence of guideline-based statin therapy will increase over time.
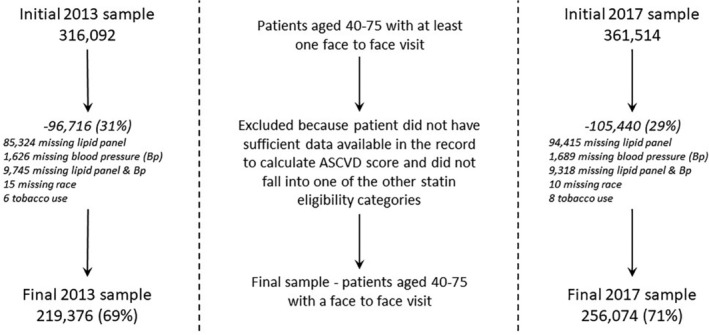
Electronic health record data were used to create two cross-sectional data sets of patients (age 40-75) served in 2013 and 2017 by a large health system. Data sets included demographics, clinical risk factors, lipid values, diagnostic codes, and active medication orders during each period. Prevalence of indications for statin therapy according to the ACC/AHA guidelines and statin prescriptions were compared between each time period.
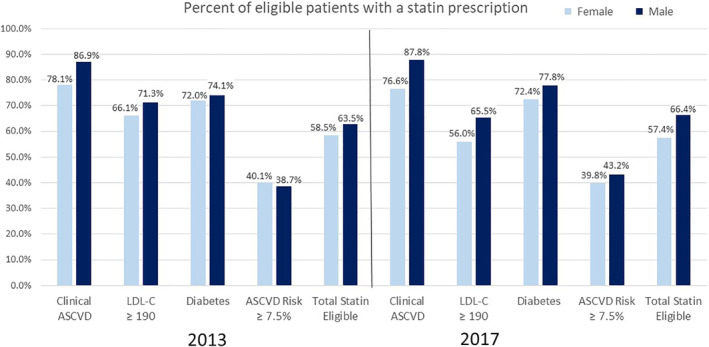
In 2013, of the 219 376 adults, 57.7% of patients met statin eligibility criteria, of which 61.3% were prescribed any statin and 19.0% a high intensity statin. Among those eligible, statin use was highest in those with established ASCVD (83.9%) and lowest in those with elevated ASCVD risk >7.5% (39.3%). In 2017, of the 256 074 adults, 62.3% were statin eligible, of which 62.3% were prescribed a statin and 24.3% a high intensity statin. In 2017, 66.4% of statin eligible men were prescribed a statin compared to 57.4% of statin eligible women (P < 0.001). The use of ezetimibe (3.6% in 2013, 2.4% in 2017) and protein convertase subtilisin/kexin type 9 inhibitors (<0.1% and 0.1%) was infrequent.
In a large health system, guideline-based statin use has remained suboptimal. Improved strategies are needed to increase statin utilization in appropriate patients.
2013年美国心脏病学会/美国心脏协会(ACC/AHA)胆固醇指南为基于动脉粥样硬化性心血管疾病(ASCVD)风险分配降脂治疗提供了循证依据。这些指南最初的采用情况并不理想,但随着时间推移情况是否有所改善仍不清楚。
基于指南的他汀类药物治疗的患病率将随时间增加。
利用电子健康记录数据创建了由一个大型医疗系统在2013年和2017年服务的两个患者(年龄40 - 75岁)横断面数据集。数据集包括每个时期的人口统计学、临床风险因素、血脂值、诊断代码和正在使用的药物医嘱。比较了每个时间段根据ACC/AHA指南的他汀类药物治疗指征患病率和他汀类药物处方情况。
2013年,在219376名成年人中,57.7%的患者符合他汀类药物治疗标准,其中61.3%的患者开具了任何他汀类药物,19.0%的患者开具了高强度他汀类药物。在符合标准的患者中,已确诊ASCVD的患者他汀类药物使用率最高(83.9%),而ASCVD风险升高>7.5%的患者使用率最低(39.3%)。2017年,在256074名成年人中,62.3%符合他汀类药物治疗标准,其中62.3%的患者开具了他汀类药物,24.3%的患者开具了高强度他汀类药物。2017年,符合他汀类药物治疗标准的男性中有66.4%开具了他汀类药物,而符合标准的女性中这一比例为57.4%(P < 0.001)。依折麦布的使用(2013年为3.6%,2017年为2.4%)和前蛋白转化酶枯草溶菌素/kexin 9型抑制剂(<0.1%和0.1%)并不常见。
在一个大型医疗系统中,基于指南的他汀类药物使用情况仍不理想。需要改进策略以提高合适患者中他汀类药物的使用率。