Department of Radiation Oncology, BC Cancer Surrey, 13750 96 Ave, Surrey, BC, V3V 1Z2, Canada.
Present Address: Department of Radiation Oncology, CHU de Québec, 11 Côte du Palais, Quebec, QC, G1R 2J6, Canada.
Radiat Oncol. 2020 Feb 27;15(1):61. doi: 10.1186/s13014-020-01491-w.
For stereotactic body radiotherapy (SBRT) to central (C) and ultracentral (UC) lung tumors, our provincial practice has been to prioritize organs at risk (OARs) constraints by compromising target volume coverage if needed. The objectives are to report the treatment's efficacy and safety.
We conducted a retrospective analysis of all provincial patients who underwent SBRT at 60Gy in 8 fractions to C and UC lung tumors, from 2013 to 2017.
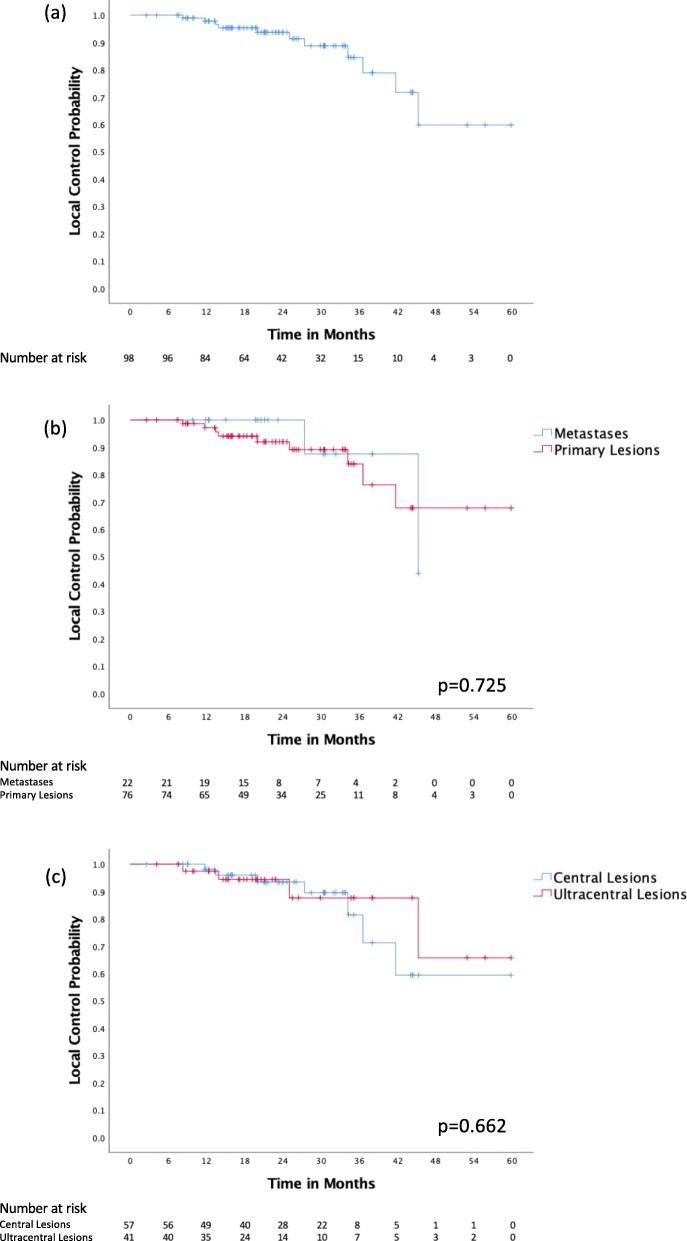
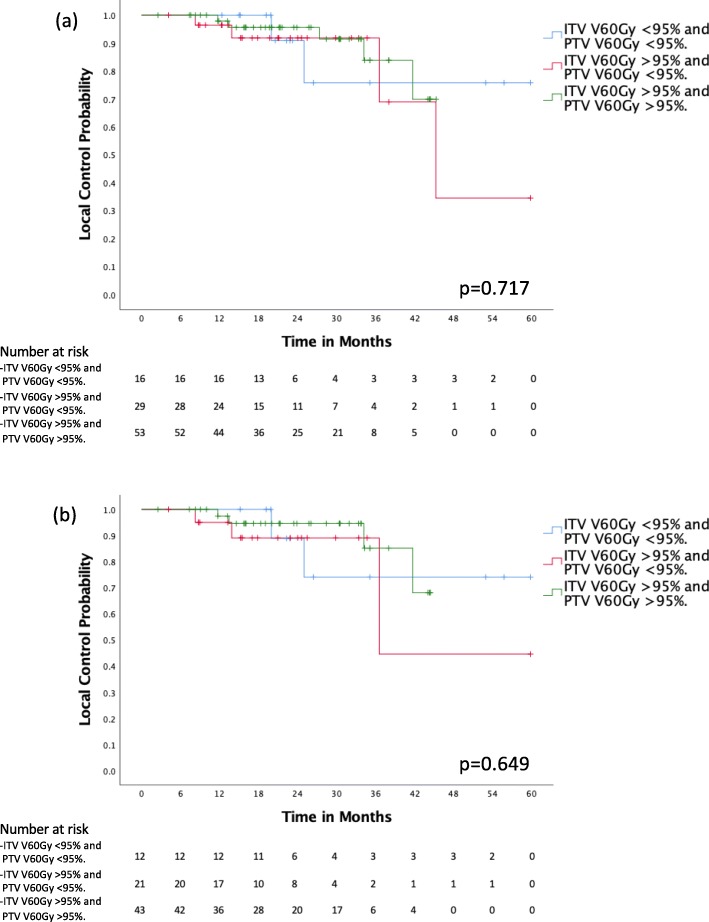
Ninety-eight lesions were treated, 57 (58.2%) C and 41 (41.8%) UC. The median follow-up was 22.9 months (range 2.5-64.8 months). The 1- and 3-year local control (LC) was 97.8 and 84.5% respectively, with no differences between C and UC groups (p = 0.662). Fifty-three (54.1%) cases had optimal dose coverage (V60Gy ITV&PTV > 95%), 29 (29.6%) had compromised PTV coverage (V60Gy ITV > 95%/PTV < 95%), and 16 (16.3%) had both compromised ITV and PTV coverage (V60Gy ITV&PTV < 95%). No significant difference in LC was detected at 2 years between the 3 groups (95.6, 91.8 and 90.9%, p = 0.717). There were 3 episodes of grade 3 toxicity in the C group (2 dyspnea, 1 pneumonitis) and 2 in the UC group (1 dyspnea, 1 hemoptysis). There were no gr4/5 toxicities. On multivariable Cox regression analysis, ITV size was found to be a predictor for LC (p = 0.001).
SBRT at 60Gy in 8 fractions achieves high rates of LC with low risks of significant toxicities, even if target volume coverage is reduced to meet OARs constraints.
对于立体定向体放射治疗(SBRT)治疗中央(C)和超中央(UC)肺部肿瘤,我们省级的做法一直是优先考虑危及器官(OARs)的限制,如果需要,可以通过妥协目标体积覆盖范围来实现。其目的是报告治疗的疗效和安全性。
我们对 2013 年至 2017 年间在 60Gy 分 8 次治疗 C 和 UC 肺部肿瘤的所有省级患者进行了回顾性分析。
共治疗了 98 个病灶,57 个(58.2%)位于 C 区,41 个(41.8%)位于 UC 区。中位随访时间为 22.9 个月(范围 2.5-64.8 个月)。1 年和 3 年局部控制率(LC)分别为 97.8%和 84.5%,C 组和 UC 组之间无差异(p=0.662)。53 例(54.1%)有最佳的剂量覆盖(V60Gy ITV&PTV>95%),29 例(29.6%)PTV 覆盖受到影响(V60Gy ITV>95%/PTV<95%),16 例(16.3%) ITV 和 PTV 覆盖均受到影响(V60Gy ITV&PTV<95%)。在 2 年时,3 组之间的 LC 差异无统计学意义(95.6%、91.8%和 90.9%,p=0.717)。C 组有 3 例 3 级毒性(2 例呼吸困难,1 例肺炎),UC 组有 2 例(1 例呼吸困难,1 例咯血)。无 4/5 级毒性。多变量 Cox 回归分析显示, ITV 大小是 LC 的预测因素(p=0.001)。
60Gy 分 8 次的 SBRT 可达到较高的局部控制率,同时毒性风险较低,即使目标体积覆盖范围缩小以满足 OARs 的限制。