Department of Orthopedic Surgery, Keio University School of Medicine, Tokyo, Japan.
Department of Orthopedic Surgery, Eiju General Hospital, Tokyo, Japan.
Clin Orthop Surg. 2020 Mar;12(1):68-75. doi: 10.4055/cios.2020.12.1.68. Epub 2020 Feb 13.
Synovial chondromatosis occurs rarely in the shoulder, and its details remain unclear. The purpose of this study was to clarify the clinical results of surgical resection and the histopathological findings of synovial chondromatosis in the shoulder.
Ten shoulders with synovial chondromatosis that had been operatively resected were reviewed retrospectively. Osteochondral lesions were present in the glenohumeral joint in six shoulders and in the subacromial space in four shoulders. Two patients had a history of trauma with glenohumeral dislocation without recurrent instability, and the other seven patients (eight shoulders) did not have any traumatic episodes or past illness involving the ipsilateral shoulder girdle. The occurrences of osteochondral lesions, inferior humeral osteophytes, and acromial spurs were assessed on radiographs before resection, just after resection, and at final follow-up. The Constant scores were compared before resection and at final follow-up with Wilcoxon signed-rank tests. Resected lesions were histopathologically differentiated between primary and secondary synovial chondromatosis.
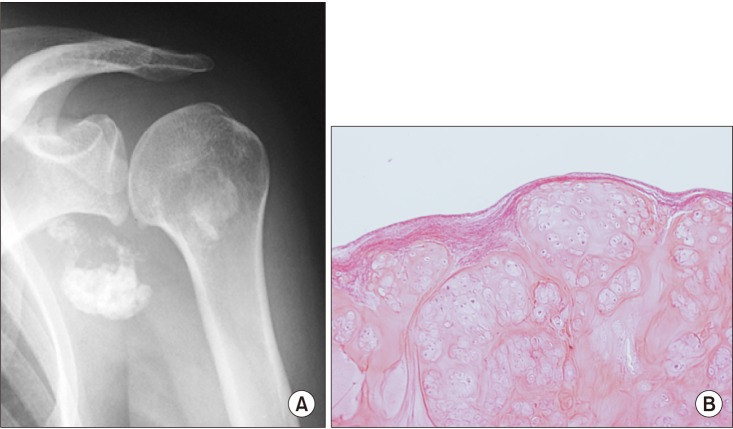
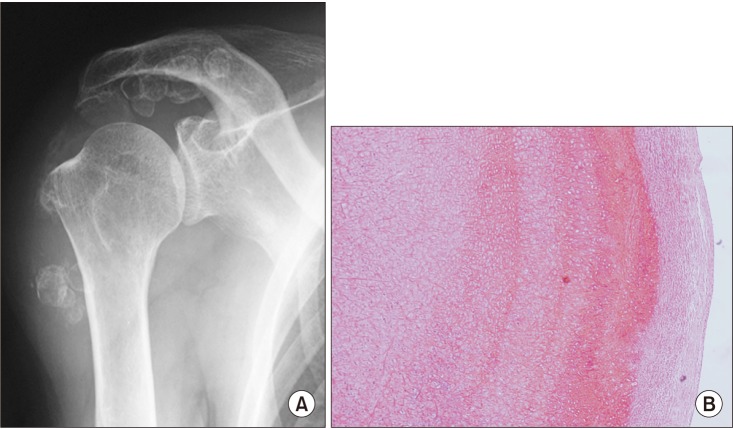
Inferior humeral osteophytes were found in five shoulders with synovial chondromatosis in the glenohumeral joint, and all four shoulders with synovial chondromatosis in the subacromial space had acromial spur formation. Osteochondral lesions appeared to have been successfully removed in all shoulders on postoperative radiographs. At the final follow-up, however, one shoulder with secondary synovial chondromatosis in the subacromial space showed recurrence of osteochondral lesions and acromial spur formation. The mean Constant score improved significantly from 53.0 points before resection to 76.0 points at a mean follow-up of 6.0 years ( = 0.002). On histopathological evaluation, one shoulder was diagnosed as having primary synovial chondromatosis, while nine shoulders had secondary synovial chondromatosis.
The present study showed that resection of shoulder osteochondral lesions successfully relieved the clinical symptoms and that primary synovial chondromatosis is less common than secondary synovial chondromatosis in the shoulder. Although most of the present osteochondral lesions were clinically determined to be primary chondromatosis, only one case was histopathologically categorized as primary synovial chondromatosis. These results suggest that histopathological identification is needed to differentiate between primary and secondary synovial chondromatosis.
滑膜软骨瘤病在肩部很少见,其细节仍不清楚。本研究旨在阐明手术切除肩部滑膜软骨瘤病的临床结果和组织病理学发现。
回顾性分析 10 例经手术切除的滑膜软骨瘤病患者。6 例盂肱关节存在骨软骨病变,4 例肩峰下间隙存在骨软骨病变。2 例患者有创伤史伴盂肱关节脱位,但无复发性不稳定,另外 7 例(8 肩)无任何创伤发作或同侧肩部既往疾病。在切除前、切除后和最终随访时评估骨软骨病变、肱骨下端骨赘和肩峰骨刺的发生情况。采用 Wilcoxon 符号秩检验比较切除前和最终随访时的 Constant 评分。对切除的病变进行组织病理学区分原发性和继发性滑膜软骨瘤病。
盂肱关节滑膜软骨瘤病 5 例出现肱骨下端骨赘,肩峰下间隙滑膜软骨瘤病 4 例均出现肩峰骨刺形成。所有肩部术后 X 线片均显示骨软骨病变已成功切除。然而,在最终随访时,1 例肩峰下间隙继发性滑膜软骨瘤病患者出现骨软骨病变和肩峰骨刺复发。Constant 评分从切除前的 53.0 分显著提高到 6.0 年平均随访时的 76.0 分(=0.002)。组织病理学评估显示,1 例诊断为原发性滑膜软骨瘤病,9 例诊断为继发性滑膜软骨瘤病。
本研究表明,切除肩部骨软骨病变可成功缓解临床症状,且原发性滑膜软骨瘤病较肩部继发性滑膜软骨瘤病少见。虽然目前大多数骨软骨病变临床上被确定为原发性软骨瘤病,但只有 1 例被组织病理学分类为原发性滑膜软骨瘤病。这些结果表明需要组织病理学鉴定来区分原发性和继发性滑膜软骨瘤病。