Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Department of Cardiothoracic and Vascular Surgery, Chang Gung Memorial Hospital, Linkou Medical Center, Taoyuan, Taiwan.
PLoS One. 2020 Mar 2;15(3):e0229648. doi: 10.1371/journal.pone.0229648. eCollection 2020.
Hemopericardium is a common and hazardous complication of acute type A aortic dissection (ATAAD). This retrospective study aimed to clarify the short-term and mid-term outcomes in patients who underwent surgical rescues for hemopericardium complicated by ATAAD.
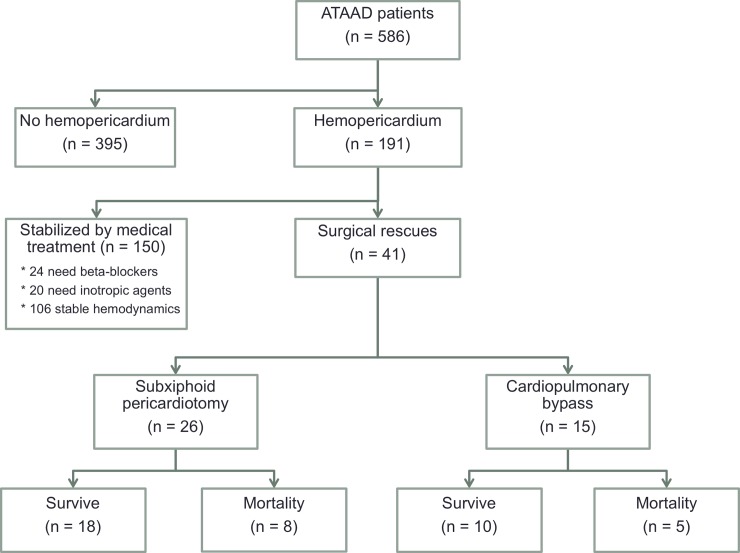
Between January 2007 and March 2019, 586 consecutive patients underwent ATAAD repair at our institution. According to preoperative computed tomography, hemopericardium was found in 191 patients (32.6%), 150 were stabilized with medical treatment, and 41 underwent surgical rescues for critical hemodynamics. The 41 patients were classified into groups according to their rescue procedures: emergent subxiphoid pericardiotomy (E-SXP group, n = 26, 63.4%) or emergent cardiopulmonary bypass (E-CPB group, n = 15, 36.6%). Clinical features, surgical information, postoperative complications, and 3-year survival were analyzed and compared.
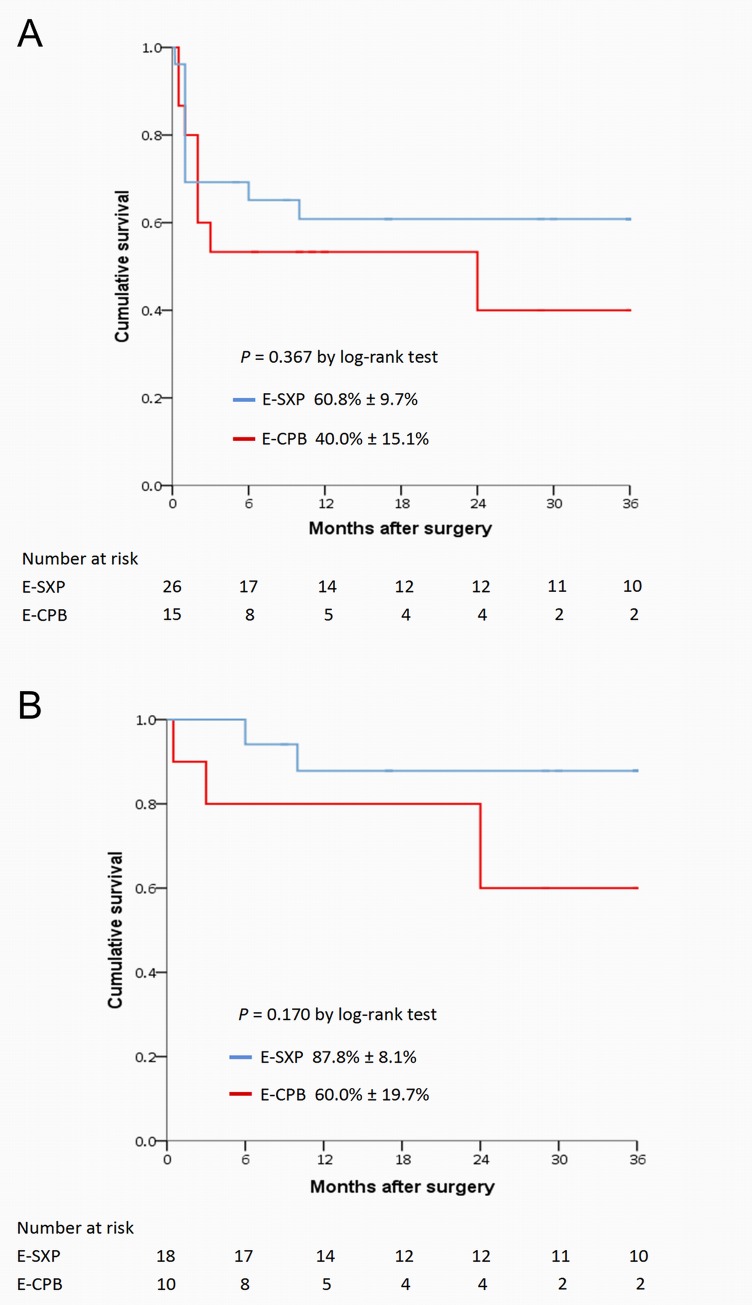
Demographics, comorbidities and aortic repair procedures were generally homogenous between the two groups, except for sex. The average systolic blood pressure was 62.4 ± 13.3 mmHg and 67.1 ± 13.1 mmHg in the E-SXP and E-CPB groups, respectively. A total of 29.3% of patients underwent cardiopulmonary resuscitation (CPR) before surgical rescues. The in-hospital mortality was similar (30.8% versus 33.3%, P = 0.865) in the two groups. Multivariate analysis revealed that preoperative CPR was an in-hospital predictor of mortality. For patients who survived to discharge, 3-year cumulative survival rates were 87.8% ± 8.1% and 60.0% ± 19.7% in the E-SXP and E-CPB groups, respectively (P = 0.170).
Patients who underwent surgical rescues for ATAAD-complicated hemopericardium are at a high risk of in-hospital mortality. The two rescue procedures revealed similar short-term and mid-term outcomes.
血心包是急性 A 型主动脉夹层(ATAAD)的常见且危险的并发症。本回顾性研究旨在阐明因 ATAAD 并发血心包而行手术抢救的患者的短期和中期结局。
2007 年 1 月至 2019 年 3 月期间,我院连续收治 586 例 ATAAD 患者。根据术前计算机断层扫描,191 例患者(32.6%)发现血心包,其中 150 例经药物稳定治疗,41 例因严重血流动力学障碍而行手术抢救。41 例患者根据抢救方式分为亚急诊经剑突下心包切开术(E-SXP 组,n=26,63.4%)或急诊体外循环(E-CPB 组,n=15,36.6%)组。分析并比较两组患者的临床特征、手术信息、术后并发症和 3 年生存率。
两组患者的一般人口统计学、合并症和主动脉修复手术过程基本相似,除性别外。E-SXP 组和 E-CPB 组的平均收缩压分别为 62.4±13.3mmHg 和 67.1±13.1mmHg。在接受手术抢救前,共有 29.3%的患者接受心肺复苏(CPR)。两组患者院内死亡率相似(30.8%比 33.3%,P=0.865)。多因素分析显示,术前 CPR 是院内死亡的预测因素。对于存活至出院的患者,E-SXP 组和 E-CPB 组的 3 年累积生存率分别为 87.8%±8.1%和 60.0%±19.7%(P=0.170)。
因 ATAAD 并发血心包而行手术抢救的患者院内死亡率较高。两种抢救方法的短期和中期结果相似。