Britt Rachel S, LaSalvia Mary T, Padival Simi, Patel Parth, McCoy Christopher, Mahoney Monica V
Department of Pharmacy, Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA.
Department of Pharmacy, The University of Texas Medical Branch, Galveston, Texas, USA.
Open Forum Infect Dis. 2019 Nov 19;6(12):ofz496. doi: 10.1093/ofid/ofz496. eCollection 2019 Dec.
Outpatient parenteral antimicrobial therapy (OPAT) allows for long-course intravenous treatment of infections without lengthy hospital stays. Upon discharge, antimicrobial therapy may be broadened for "ease" of once-daily administration (EOA). Patients requiring subsequent readmission can be tailored to pre-OPAT regimens to minimize adverse effects. This study assessed continuation of EOA regimens upon hospital readmission during or immediately after OPAT.
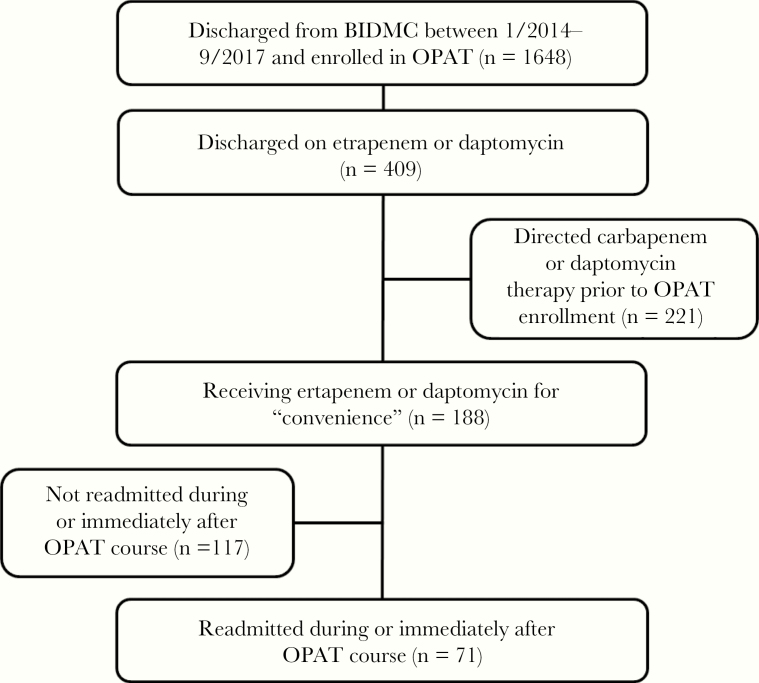
This was a retrospective review of adults enrolled in OPAT and discharged on ertapenem or daptomycin for EOA, defined by the terms "convenience" or "EOA" in OPAT notes or by switching to ertapenem or daptomycin upon OPAT enrollment despite adequate therapy with narrower-spectrum agents. The primary outcome was the percentage of patients readmitted during or after their OPAT course and maintained on an EOA regimen. Secondary outcomes included inpatient therapy cost, rates of infection, and adverse events.
Of 188 patients receiving an OPAT EOA regimen, 71 were readmitted, representing 113 unique readmissions. Patients were mostly males (81%) aged 57 years. The EOA regimens were continued in 27% of hospital readmissions. The Infectious Diseases (ID) team was consulted in 48% of readmissions, and the Antimicrobial Stewardship Program (ASP) intervened in 26%. Combined, this resulted in de-escalation in 28% of cases. infections and adverse events occurred in 7% and 12% of readmissions, respectively. The median acquisition cost of inpatient EOA regimens was $150 per readmission.
The OPAT EOA regimens were continued in 27% of hospital readmissions indicating a role for improved indication documentation and collaboration between ID services, ASPs, and OPAT teams.
门诊胃肠外抗菌治疗(OPAT)可在无需长时间住院的情况下对感染进行长期静脉治疗。出院时,抗菌治疗可因每日一次给药“方便”(EOA)而扩大范围。需要再次入院的患者可采用OPAT前的治疗方案,以尽量减少不良反应。本研究评估了在OPAT期间或之后立即再次入院时EOA方案的延续情况。
这是一项对参加OPAT并因EOA而接受厄他培南或达托霉素出院的成年人的回顾性研究,EOA在OPAT记录中由“方便”或“EOA”定义,或在OPAT登记时尽管使用窄谱药物进行了充分治疗但仍改用厄他培南或达托霉素。主要结局是在OPAT疗程期间或之后再次入院并维持EOA方案的患者百分比。次要结局包括住院治疗费用、感染率和不良事件。
在188例接受OPAT EOA方案的患者中,71例再次入院,代表113次单独的再次入院。患者大多为男性(81%),年龄57岁。27%的再次入院患者继续使用EOA方案。48%的再次入院患者咨询了传染病(ID)团队,26%的患者抗菌管理计划(ASP)进行了干预。综合起来,这导致28%的病例治疗降级。分别有7%和12%的再次入院患者发生感染和不良事件。住院EOA方案的中位采购成本为每次再次入院150美元。
27%的再次入院患者继续使用OPAT EOA方案,这表明改善指征记录以及ID服务、ASP和OPAT团队之间的协作具有重要作用。