Department of Anesthesiology and Intensive Care Medicine, Essen University Hospital, Essen, Germany.
Department of Anesthesiology and Intensive Care Medicine, Heidelberg University Hospital, Heidelberg, Germany.
World J Surg. 2020 Jul;44(7):2295-2304. doi: 10.1007/s00268-020-05444-y.
Atrial fibrillation (AF) represents the most frequent arrhythmic disorder after thoracoabdominal esophageal resection and is associated with a significant increase in perioperative morbidity and mortality.
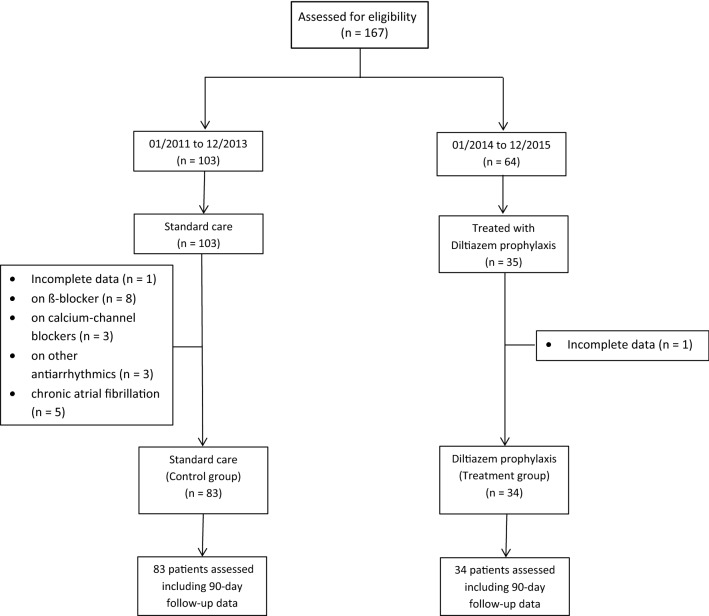
In this retrospective cohort study, 167 patients who underwent thoracoabdominal esophagectomy at a large university hospital were assessed. We compared patients who received a 14-day postoperative course of diltiazem with a control group of patients who did not undergo diltiazem prophylaxis. Diltiazem therapy started immediately upon admission to the intensive care unit (ICU) with a loading dose of 0.25 mg/kg bodyweight (i.v.) followed by continuous infusion (0.1 mg/kg bodyweight/h) for 40-48 h. Oral administration (Dilzem 180 mg uno retard, once a day) was started on postoperative day 3.
A total of 117 patients were assessed. Twelve (10.3%) of all patients developed postoperative new-onset atrial fibrillation in the first 30 days after surgical intervention. Prevalence of new-onset AF showed no significant differences between the diltiazem group and control group (p = 0.74). The prevalence of bradycardia (14.7% vs. 3.6%; p = 0.03) and dose of norepinephrine required (0.09 vs. 0.04 µg/kg bodyweight/min; p = 0.04) were higher in the diltiazem group. There were no significant differences between the groups for the median postoperative duration of hospital/ICU stay or mortality.
A prophylactic 14-day postoperative course of diltiazem was not associated with a reduction in new-onset AF or 30-day mortality following thoracoabdominal esophagectomy. Prophylactic diltiazem therapy was associated with drug-related adverse effects such as bradycardia and increased requirement of norepinephrine. German Clinical Trial Registration Number: DKRS00016631.
心房颤动(AF)是胸腹食管切除术后最常见的心律失常,与围手术期发病率和死亡率的显著增加有关。
在这项回顾性队列研究中,评估了在一家大型大学医院接受胸腹食管切除术的 167 名患者。我们比较了接受地尔硫䓬术后 14 天疗程的患者和未接受地尔硫䓬预防治疗的对照组患者。地尔硫䓬治疗在入住重症监护病房(ICU)时立即开始,给予 0.25mg/kg 体重的负荷剂量(静脉注射),然后连续输注(0.1mg/kg 体重/小时)40-48 小时。术后第 3 天开始口服(Dilzem 180mg uno retard,每天一次)。
共评估了 117 名患者。所有患者中有 12 名(10.3%)在手术干预后 30 天内出现新发的术后心房颤动。地尔硫䓬组和对照组新发 AF 的发生率无显著差异(p=0.74)。地尔硫䓬组心动过缓(14.7%比 3.6%;p=0.03)和去甲肾上腺素需要量(0.09比 0.04μg/kg 体重/分钟;p=0.04)较高。两组患者的术后住院/ICU 时间中位数或死亡率无显著差异。
胸腹食管切除术后预防性应用地尔硫䓬 14 天疗程并不能降低新发心房颤动或 30 天死亡率。预防性地尔硫䓬治疗与药物相关的不良反应有关,如心动过缓和去甲肾上腺素需求增加。德国临床试验注册编号:DKRS00016631。