Ethiopian Public Health Institute, Arbegnoch Street, Mail Box: 19922, Addis Ababa, Ethiopia.
School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia.
Malar J. 2020 Mar 4;19(1):108. doi: 10.1186/s12936-020-03177-w.
Ethiopia has set a goal for malaria elimination by 2030. Low parasite density infections may go undetected by conventional diagnostic methods (microscopy and rapid diagnostic tests) and their contribution to malaria transmission varies by transmission settings. This study quantified the burden of subpatent infections from samples collected from three regions of northwest Ethiopia.
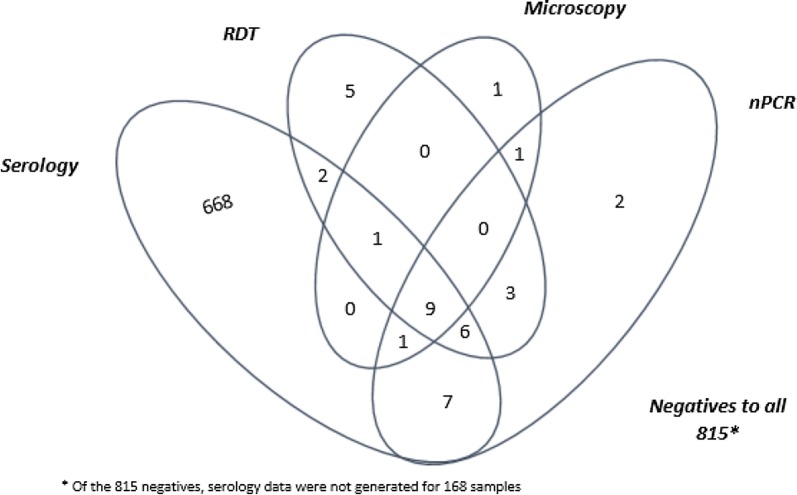
Sub-samples of dried blood spots from the Ethiopian Malaria Indicator Survey 2015 (EMIS-2015) were tested and compared using microscopy, rapid diagnostic tests (RDTs), and nested polymerase chain reaction (nPCR) to determine the prevalence of subpatent infection. Paired seroprevalence results previously reported along with gender, age, and elevation of residence were explored as risk factors for Plasmodium infection.
Of the 2608 samples collected, the highest positive rate for Plasmodium infection was found with nPCR 3.3% (95% CI 2.7-4.1) compared with RDT 2.8% (95% CI 2.2-3.5) and microscopy 1.2% (95% CI 0.8-1.7). Of the nPCR positive cases, Plasmodium falciparum accounted for 3.1% (95% CI 2.5-3.8), Plasmodium vivax 0.4% (95% CI 0.2-0.7), mixed P. falciparum and P. vivax 0.1% (95% CI 0.0-0.4), and mixed P. falciparum and Plasmodium malariae 0.1% (95% CI 0.0-0.3). nPCR detected an additional 30 samples that had not been detected by conventional methods. The majority of the nPCR positive cases (61% (53/87)) were from the Benishangul-Gumuz Region. Malaria seropositivity had significant association with nPCR positivity [adjusted OR 10.0 (95% CI 3.2-29.4), P < 0.001].
Using nPCR the detection rate of malaria parasites increased by nearly threefold over rates based on microscopy in samples collected during a national cross-sectional survey in 2015 in Ethiopia. Such subpatent infections might contribute to malaria transmission. In addition to strengthening routine surveillance systems, malaria programmes may need to consider low-density, subpatent infections in order to accelerate malaria elimination efforts.
埃塞俄比亚设定了到 2030 年消除疟疾的目标。低寄生虫密度感染可能会被常规诊断方法(显微镜和快速诊断检测)漏诊,其对疟疾传播的贡献因传播环境而异。本研究定量评估了来自埃塞俄比亚西北部三个地区的样本中亚临床感染的负担。
使用显微镜、快速诊断检测(RDT)和巢式聚合酶链反应(nPCR)对 2015 年埃塞俄比亚疟疾指标调查(EMIS-2015)的亚样本进行检测和比较,以确定亚临床感染的流行率。以前报告的血清阳性率以及性别、年龄和居住地海拔高度被探索为感染疟原虫的危险因素。
在采集的 2608 个样本中,nPCR 的疟原虫感染阳性率最高,为 3.3%(95%CI 2.7-4.1),而 RDT 为 2.8%(95%CI 2.2-3.5),显微镜为 1.2%(95%CI 0.8-1.7)。nPCR 阳性病例中,恶性疟原虫占 3.1%(95%CI 2.5-3.8),间日疟原虫占 0.4%(95%CI 0.2-0.7),恶性疟原虫和间日疟原虫混合感染占 0.1%(95%CI 0.0-0.4),恶性疟原虫和疟原虫混合感染占 0.1%(95%CI 0.0-0.3)。nPCR 检测到常规方法未检测到的额外 30 个样本。nPCR 阳性病例的大多数(61%(53/87))来自本尚古勒-古马兹州。疟疾血清阳性与 nPCR 阳性有显著关联[调整后的比值比 10.0(95%CI 3.2-29.4),P<0.001]。
在 2015 年埃塞俄比亚进行的全国横断面调查中,使用 nPCR 检测疟原虫的检出率比基于显微镜的检测率高出近三倍。这种亚临床感染可能会促进疟疾传播。除了加强常规监测系统外,疟疾规划可能还需要考虑低密度、亚临床感染,以加速消除疟疾的努力。