Zheng Yajuan, Zhong Guansheng, Yu Kun, Lei Kefeng, Yang Qiong
Department of Breast and Thyroid Surgery, Zhejiang Provincial People's Hospital, People's Hospital of Hangzhou Medical College, Hangzhou, China.
Department of Breast Surgery, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China.
Front Oncol. 2020 Feb 18;10:148. doi: 10.3389/fonc.2020.00148. eCollection 2020.
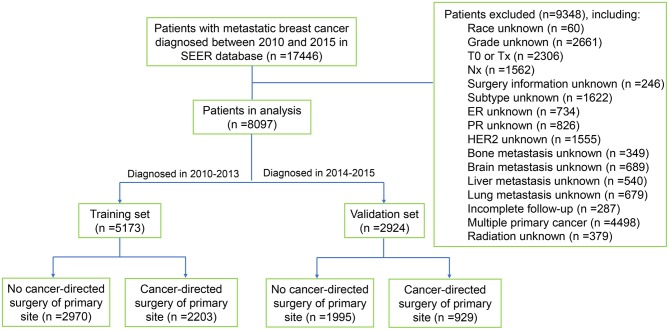
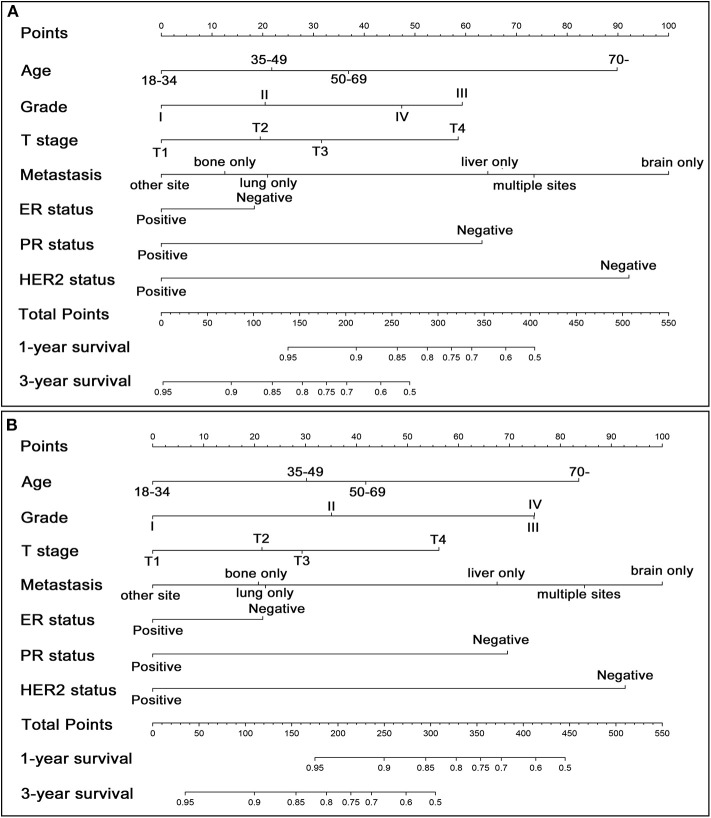
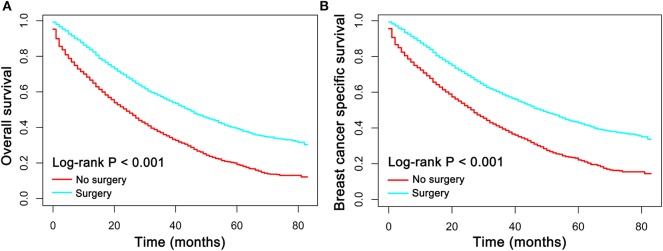
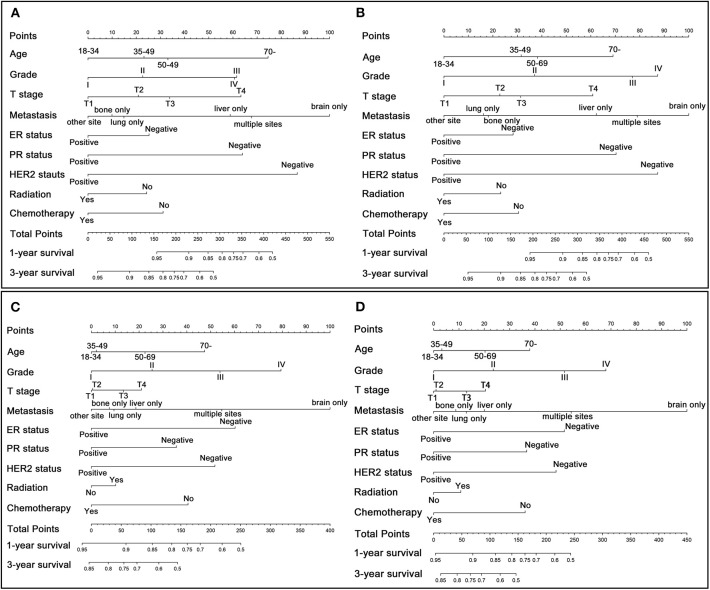
Recently, performing locoregional surgical treatment still remains debatable in patients with metastatic breast cancer (MBC). Current study aimed to develop prognostic nomograms for predicting the long-term survival in MBC patients with or without surgical intervention, thereby assisting clinicians in making individualized choice. The training set included 5173 patients who were diagnosed with MBC in 2010-2013 from the Surveillance, Epidemiology, and End Results Program, while the validation set comprised 2924 patients diagnosed in 2014-2015. Multivariant Cox hazard model was applied to determine the independent risk factors for overall survival (OS) and breast cancer specific survival (BCSS). Then, individualized pre- and postoperative nomograms for predicting 1- or 3-year survival probabilities were constructed accordingly. Internal and external validations were conducted to determine the accuracy of these nomograms by calculating concordance index (C-index) and plotting calibration curves. The survival analysis indicated that surgical management conferred improved OS and BCSS in patients with metastatic breast cancer. Age, T stage, grade, distant metastatic site, ER, PR and HER2 status, radiation, and chemotherapy were independent risk factors for OS and BCSS both in surgery and non-surgery group. All these factors were subsequently incorporated into the nomogram which showed acceptable predictive capabilities with C-index range of 0.65-0.80 both in training set and external validation set. In addition, a preoperative nomogram incorporating variables capable of being determined before surgery was also built with C-index above 0.70 both in training and validation set. Surgical management in patients with metastatic breast cancer suggests a potential survival advantage. In addition, these well-validated pre- and postoperative nomograms may provide a useful tool to assist clinicians in treatment decision-making and in evaluating patients' long term prognosis.
最近,对于转移性乳腺癌(MBC)患者而言,进行局部区域手术治疗仍存在争议。当前研究旨在开发预后列线图,以预测接受或未接受手术干预的MBC患者的长期生存情况,从而帮助临床医生做出个体化选择。训练集包括2010年至2013年期间从监测、流行病学和最终结果计划中诊断为MBC的5173例患者,而验证集包括2014年至2015年期间诊断的2924例患者。应用多变量Cox风险模型来确定总生存(OS)和乳腺癌特异性生存(BCSS)的独立危险因素。然后,据此构建用于预测1年或3年生存概率的个体化术前和术后列线图。通过计算一致性指数(C指数)和绘制校准曲线进行内部和外部验证,以确定这些列线图的准确性。生存分析表明,手术治疗可改善转移性乳腺癌患者的OS和BCSS。年龄、T分期、分级、远处转移部位、雌激素受体(ER)、孕激素受体(PR)和人表皮生长因子受体2(HER2)状态、放疗和化疗是手术组和非手术组中OS和BCSS的独立危险因素。所有这些因素随后都被纳入列线图,该列线图在训练集和外部验证集中均显示出可接受的预测能力,C指数范围为0.65至0.80。此外,还构建了一个术前列线图,纳入了术前能够确定的变量,在训练集和验证集中C指数均高于0.70。转移性乳腺癌患者的手术治疗显示出潜在的生存优势。此外,这些经过充分验证的术前和术后列线图可能为临床医生提供一个有用的工具,以协助治疗决策和评估患者的长期预后。