From the Neuromuscular Diseases Unit (X.S.-C., J.A.-P., A.C.-R., E.F.-S., A.A.-J., R.R.-G., J.T., L.Q., N.d.L., E.C.-V., I.I., E.G., J.D.-M.), Neurology Department, Hospital de la Santa CreuiSant Pau and Biomedical Research Institute Sant Pau (IIB Sant Pau), Barcelona; Centro de Investigaciones Biomédicas en Red en Enfermedades Raras (CIBERER) (X.S.-C., R.R.-G., L.Q., N.d.L., E.C.-V., I.I., E.G., J.D.-M.), Madrid; John Walton Muscular Dystrophy Research Center (J.D.-M), University of Newcastle, UK; Rheumatology Unit (I.C., A.M.-n.-M., H.C.), Hospital de la Santa Creu i Sant Pau; Laboratory of Experimental Immunology (C.Z.), Hospital de la Santa Creu i Sant Pau, Biomedical Research Institute Sant Pau (IIB Sant Pau); Servei Immunologia (L.M.-M.), Hospital de la Santa Creu i Sant Pau, Biomedical Research Institute Sant Pau (IIB Sant Pau); and Department of Respiratory Medicine (D.C.), Hospital de la Santa Creu i Sant Pau, Barcelona, Spain.
Neurol Neuroimmunol Neuroinflamm. 2020 Mar 6;7(3). doi: 10.1212/NXI.0000000000000694. Print 2020 May.
To describe the clinical, serologic and histologic features of a cohort of patients with brachio-cervical inflammatory myopathy (BCIM) associated with systemic sclerosis (SSc) and unravel disease-specific pathophysiologic mechanisms occurring in these patients.
We reviewed clinical, immunologic, muscle MRI, nailfold videocapillaroscopy, muscle biopsy, and response to treatment data from 8 patients with BCIM-SSc. We compared cytokine profiles between patients with BCIM-SSc and SSc without muscle involvement and controls. We analyzed the effect of the deregulated cytokines in vitro (fibroblasts, endothelial cells, and muscle cells) and in vivo.
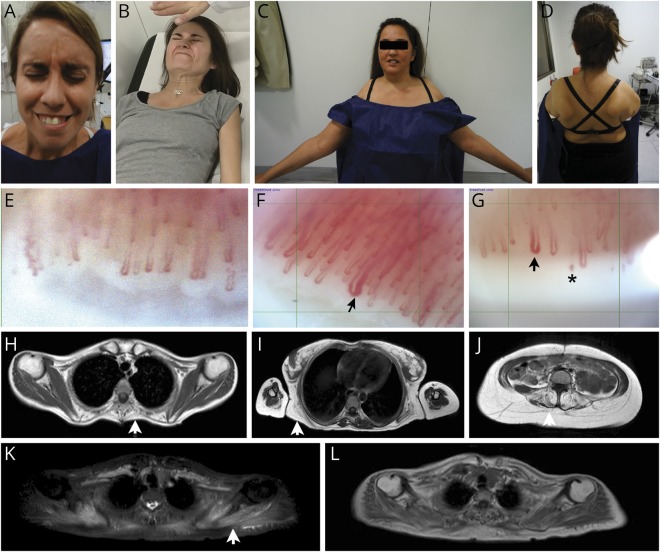
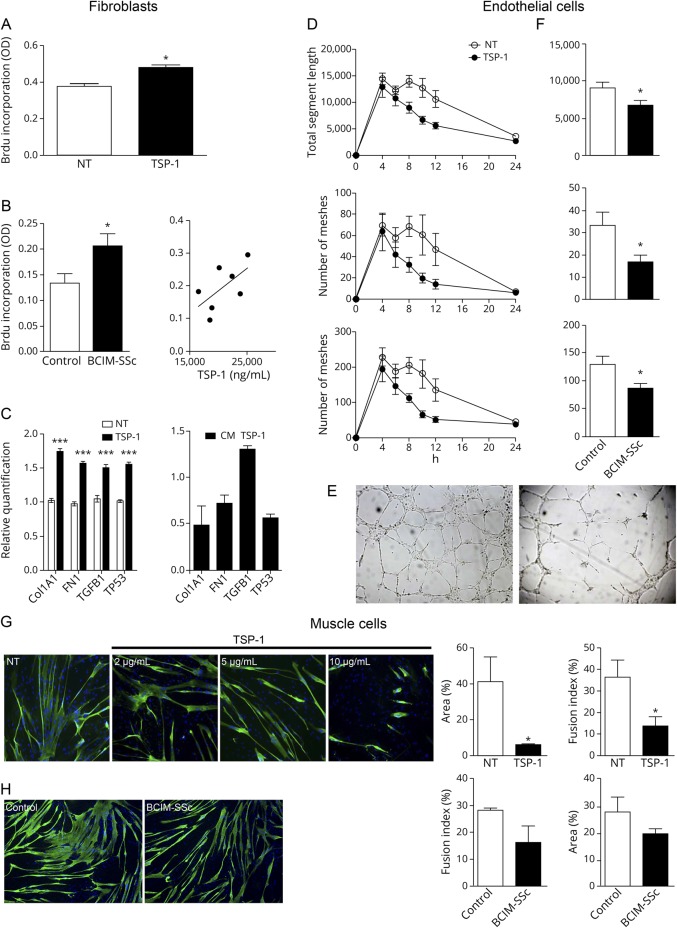
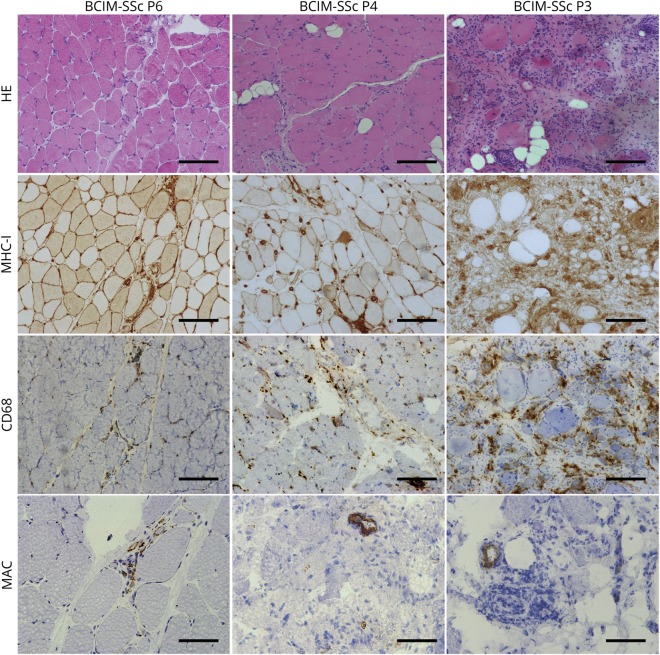
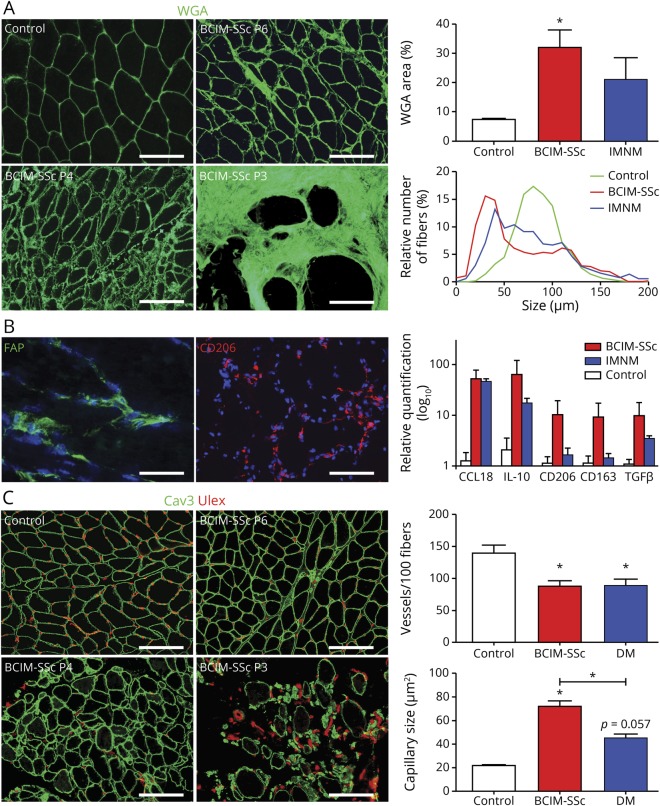
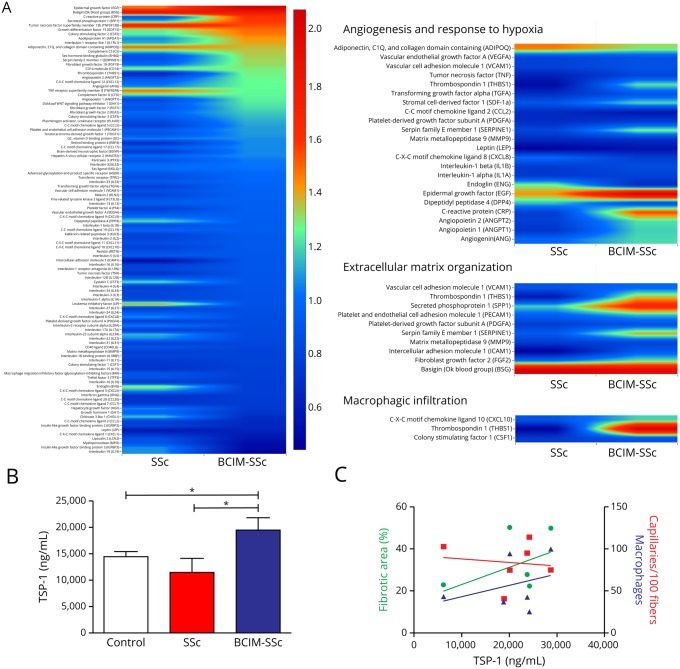
All patients with BCIM-SSc presented with muscle weakness involving cervical and proximal muscles of the upper limbs plus Raynaud syndrome, telangiectasia and/or sclerodactilia, hypotonia of the esophagus, and interstitial lung disease. Immunosuppressive treatment stopped the progression of the disease. Muscle biopsy showed pathologic changes including the presence of necrotic fibers, fibrosis, and reduced capillary number and size. Cytokines involved in inflammation, angiogenesis, and fibrosis were deregulated. Thrombospondin-1 (TSP-1), which participates in all these 3 processes, was upregulated in patients with BCIM-SSc. In vitro, TSP-1 and serum of patients with BCIM-SSc promoted proliferation and upregulation of collagen, fibronectin, and transforming growth factor beta in fibroblasts. TSP-1 disrupted vascular network, decreased muscle differentiation, and promoted hypotrophic myotubes. In vivo, TSP-1 increased fibrotic tissue and profibrotic macrophage infiltration in the muscle.
Patients with SSc may present with a clinically and pathologically distinct myopathy. A prompt and correct diagnosis has important implications for treatment. Finally, TSP-1 may participate in the pathologic changes observed in muscle.
描述与系统性硬化症(SSc)相关的臂颈炎性肌病(BCIM)患者的临床、血清学和组织学特征,并阐明这些患者中发生的特定于疾病的病理生理机制。
我们回顾了 8 例 BCIM-SSc 患者的临床、免疫、肌肉 MRI、甲襞视频毛细血管镜、肌肉活检和治疗反应数据。我们比较了 BCIM-SSc 患者与无肌肉受累的 SSc 患者和对照组之间的细胞因子谱。我们分析了体外(成纤维细胞、内皮细胞和肌细胞)和体内失调细胞因子的影响。
所有 BCIM-SSc 患者均出现上肢颈和近端肌肉无力,伴有雷诺综合征、毛细血管扩张和/或硬皮病、食管张力减退和间质性肺病。免疫抑制治疗阻止了疾病的进展。肌肉活检显示存在病理改变,包括坏死纤维、纤维化以及毛细血管数量和大小减少。涉及炎症、血管生成和纤维化的细胞因子失调。参与所有这 3 个过程的血小板反应蛋白-1(TSP-1)在 BCIM-SSc 患者中上调。在体外,TSP-1 和 BCIM-SSc 患者的血清促进成纤维细胞中胶原蛋白、纤维连接蛋白和转化生长因子β的增殖和上调。TSP-1 破坏血管网络,减少肌肉分化,并促进萎缩肌管。在体内,TSP-1 增加了肌肉中的纤维组织和促纤维化巨噬细胞浸润。
SSc 患者可能表现出具有临床和病理特征的肌病。及时和正确的诊断对治疗具有重要意义。最后,TSP-1 可能参与了肌肉中观察到的病理变化。