van Wessem Karlijn J P, Hietbrink Falco, Leenen Luke P H
Department of Trauma Surgery, University Medical Center Utrecht, Utrecht, The Netherlands.
Trauma Surg Acute Care Open. 2020 Feb 4;5(1):e000398. doi: 10.1136/tsaco-2019-000398. eCollection 2020.
The recent decrease in multiple organ dysfunction syndrome (MODS)-associated and adult respiratory distress syndrome (ARDS)-associated mortality could be considered a success of improvements in trauma care. However, the incidence of infections remains high in patients with polytrauma, with high morbidity and hospital resources usage. Infectious complications might be a residual effect of the decrease in MODS-related/ARDS-related mortality. This study investigated the current incidence of infectious complications in polytrauma.
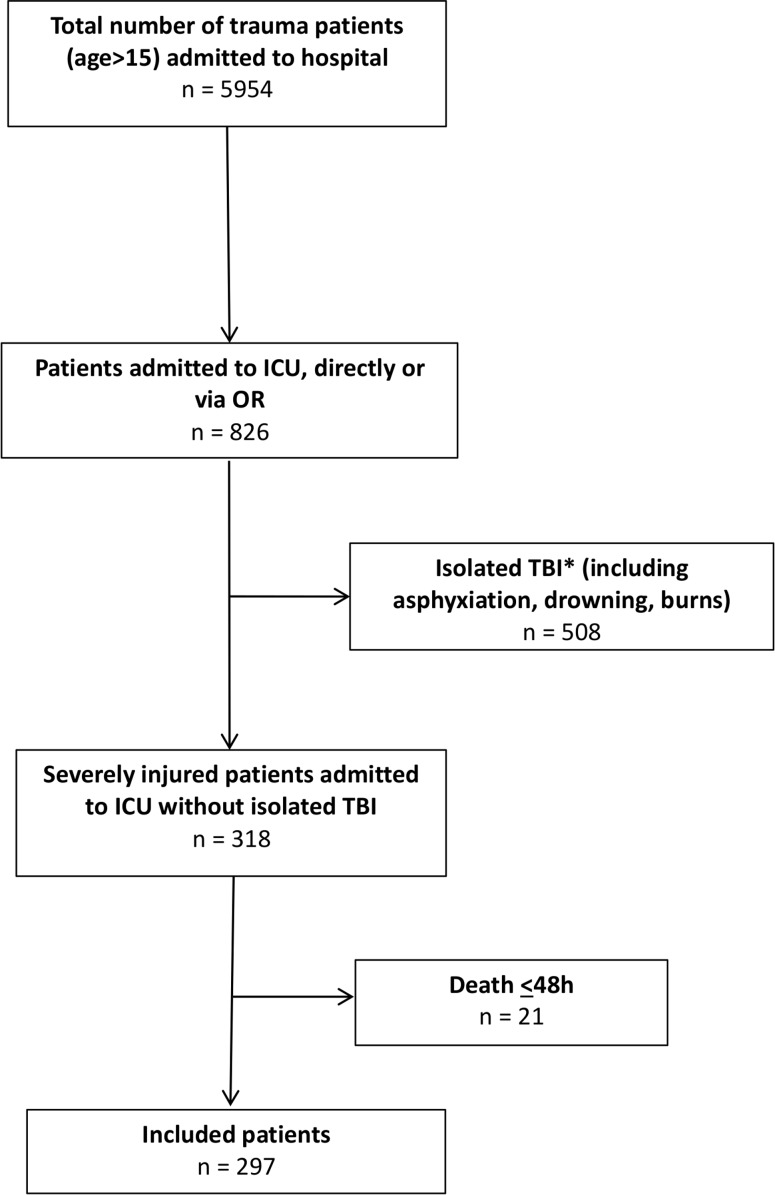
A 5.5-year prospective population-based cohort study included consecutive severely injured patients (age >15) admitted to a (Level-1) trauma center intensive care unit (ICU) who survived >48 hours. Demographics, physiologic and resuscitation parameters, multiple organ failure and ARDS scores, and infectious complications (pneumonia, fracture-related infection, meningitis, infections related to blood, wound, and urinary tract) were prospectively collected. Data are presented as median (IQR), p<0.05 was considered significant.
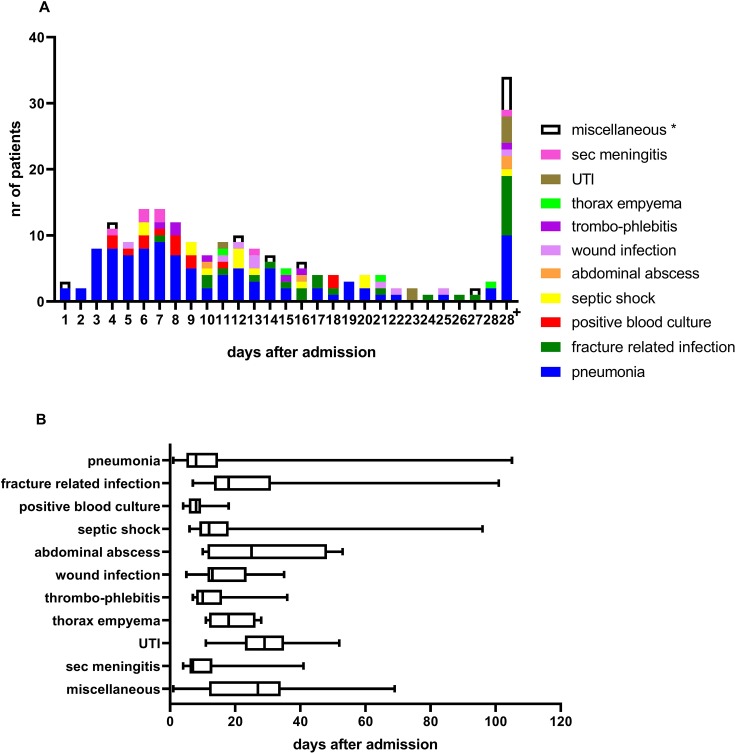
297 patients (216 (73%) men) were included with median age of 46 (27-60) years, median Injury Severity Score was 29 (22-35), 96% sustained blunt injuries. 44 patients (15%) died. One patient (2%) died of MODS and 1 died of ARDS. 134 patients (45%) developed 201 infectious complications. Pneumonia was the most common complication (50%). There was no difference in physiologic parameters on arrival in emergency department and ICU between patients with and without infectious complications. Patients who later developed infections underwent more often a laparotomy (32% vs 18%, p=0.009), had more often pelvic fractures (38% vs 25%, p=0.02), and received more blood products <8 hours. They had more often MODS (25% vs 13%, p=0.005), stayed longer on the ventilator (10 (5-15) vs 5 (2-8) days, p<0.001), longer in ICU (11 (6-17) vs 6 (3-10) days, p<0.001), and in hospital (30 (20-44) vs 16 (10-24) days, p<0.001). There was however no difference in mortality (12% vs 17%, p=0.41) between both groups.
45% of patients developed infectious complications. These patients had similar mortality rates, but used more hospital resources. With low MODS-related and ARDS-related mortality, infections might be a residual effect, and are one of the remaining challenges in the treatment of patients with polytrauma.
Level 3.
Population-based cohort study.
多器官功能障碍综合征(MODS)和成人呼吸窘迫综合征(ARDS)相关死亡率最近有所下降,这可被视为创伤护理改善的一项成功。然而,多发伤患者的感染发生率仍然很高,发病率和医院资源使用率也很高。感染并发症可能是MODS相关/ARDS相关死亡率下降的残留效应。本研究调查了多发伤患者目前感染并发症的发生率。
一项为期5.5年的基于人群的前瞻性队列研究,纳入了连续入住(一级)创伤中心重症监护病房(ICU)且存活超过48小时的严重受伤患者(年龄>15岁)。前瞻性收集人口统计学、生理和复苏参数、多器官功能衰竭和ARDS评分以及感染并发症(肺炎、骨折相关感染、脑膜炎、血液、伤口和尿路感染)。数据以中位数(四分位间距)表示,p<0.05被认为具有统计学意义。
纳入297例患者(216例(73%)为男性),中位年龄46(27 - 60)岁,中位损伤严重度评分29(22 - 35),96%为钝性损伤。44例(15%)患者死亡。1例(2%)死于MODS,1例死于ARDS。134例(45%)患者发生了201例感染并发症。肺炎是最常见的并发症(50%)。有感染并发症和无感染并发症的患者到达急诊科和ICU时的生理参数无差异。后来发生感染的患者更常接受剖腹手术(32%对18%,p = 0.009),更常发生骨盆骨折(38%对25%,p = 0.02),且在8小时内接受更多血液制品。他们更常发生MODS(25%对13%,p = 0.005),机械通气时间更长(10(5 - 15)天对5(2 - 8)天,p<0.001),在ICU停留时间更长(11(6 - 17)天对6(3 - 10)天,p<0.001),住院时间更长(30(20 - 44)天对16(10 - 24)天,p<0.001)。然而,两组之间的死亡率无差异(12%对17%,p = 0.41)。
45%的患者发生了感染并发症。这些患者死亡率相似,但使用了更多的医院资源。由于MODS相关和ARDS相关死亡率较低,感染可能是一种残留效应,并且是多发伤患者治疗中尚存的挑战之一。
3级。
基于人群的队列研究。