Trauma Surgeon, Department of Trauma Surgery, University Medical Center Utrecht, Utrecht, The Netherlands.
Professor of Trauma Surgery, Department of Trauma Surgery, University Medical Center Utrecht, Utrecht, the Netherlands.
Eur J Trauma Emerg Surg. 2022 Feb;48(1):357-365. doi: 10.1007/s00068-020-01567-y. Epub 2020 Dec 15.
Age in severely injured patients has been increasing for decades. Older age is associated with increasing mortality. However, morbidity and mortality could possibly be reduced when accurate and aggressive treatment is provided. This study investigated age-related morbidity and mortality in polytrauma including age-related decisions in initial injury management and withdrawal of life-sustaining therapy (WLST).
A 6.5-year prospective cohort study included consecutive severely injured trauma patients admitted to a Level-1 Trauma Center ICU. Demographics, data on physiology, resuscitation, MODS/ARDS, and infectious complications were prospectively collected. Patients were divided into age subgroups (< 25, 25-49, 50-69, and ≥ 70 years) to make clinically relevant comparisons.
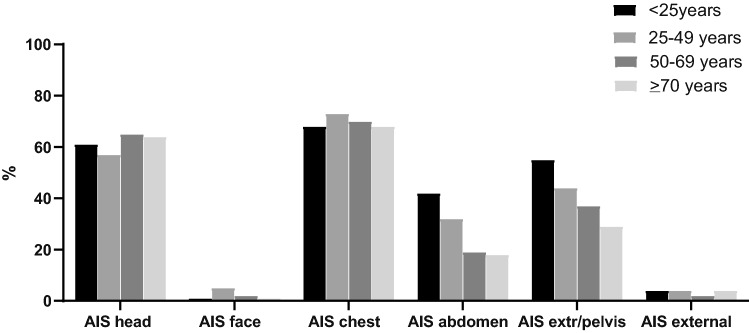
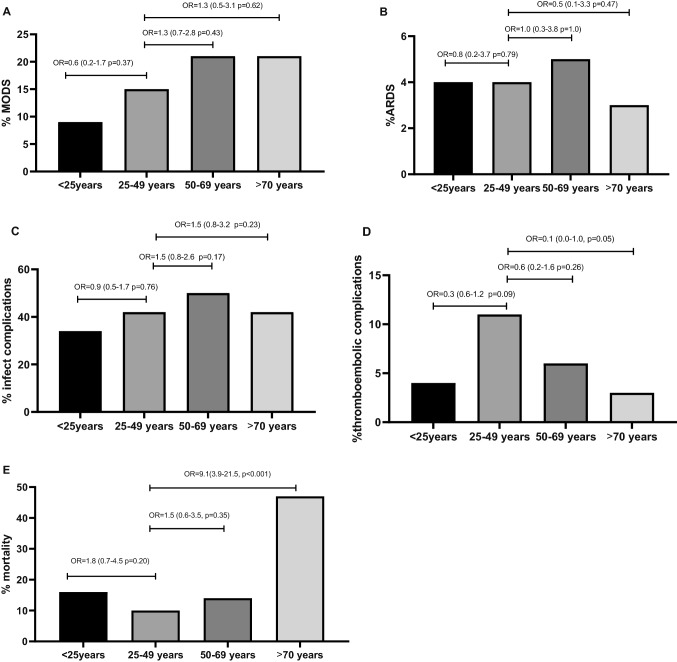
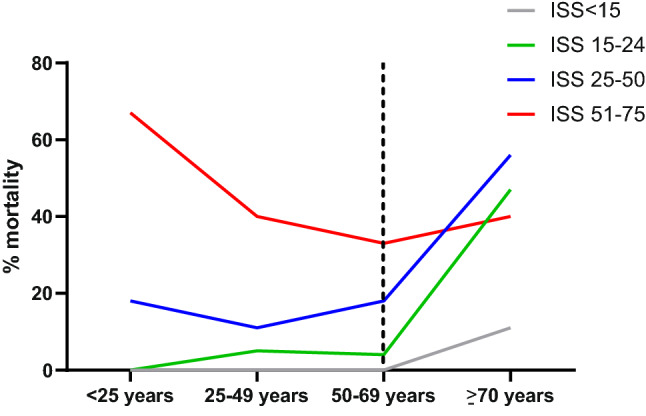
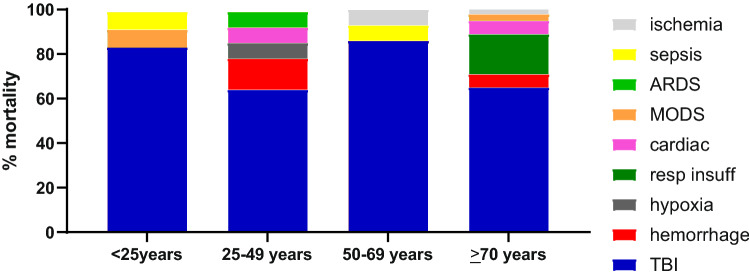
391 patients (70% males) were included with median ISS of 29 (22-36), 95% sustained blunt injuries. There was no difference in injury severity, resuscitation, urgent surgeries, nor in ventilator days, ICU-LOS, and H-LOS between age groups. Adjusted odds of MODS, ARDS and infectious complications were similar between age groups. 47% of patients ≥ 70 years died, compared to 10-16% in other age groups (P < 0.001). WLST increased with older age, contributing to more than half of deaths ≥ 70 years. TBI was the most common cause of death and decision for treatment withdrawal in all age groups.
Patients ≥ 70 years had higher mortality risk even though injury severity and complication rates were similar to other age groups. WLST increased with age with the vast majority due to brain injury. More than half of patients ≥ 70 years survived suggesting geriatric polytrauma patients should not be excluded from aggressive injury treatment based on age alone.
严重创伤患者的年龄在过去几十年中一直在增加。年龄越大,死亡率越高。然而,当提供准确和积极的治疗时,发病率和死亡率可能会降低。本研究调查了多发伤中与年龄相关的发病率和死亡率,包括初始损伤管理和终止生命支持治疗(WLST)中的年龄相关决策。
一项为期 6.5 年的前瞻性队列研究纳入了连续收入一级创伤中心 ICU 的严重创伤患者。前瞻性收集了人口统计学、生理学、复苏、MODS/ARDS 和感染并发症的数据。患者被分为年龄亚组(<25 岁、25-49 岁、50-69 岁和≥70 岁),以进行临床相关比较。
纳入 391 例(70%为男性)患者,ISS 中位数为 29(22-36),95%为钝性损伤。年龄组之间的损伤严重程度、复苏、紧急手术以及呼吸机使用天数、ICU 住院时间和住院时间无差异。调整后的 MODS、ARDS 和感染并发症的发生几率在各年龄组之间相似。≥70 岁的患者中有 47%死亡,而其他年龄组的死亡率为 10-16%(P<0.001)。随着年龄的增长,WLST 增加,导致≥70 岁的患者死亡超过一半。TBI 是所有年龄组中最常见的死亡原因和治疗终止决策。
即使损伤严重程度和并发症发生率与其他年龄组相似,≥70 岁的患者死亡风险仍然较高。随着年龄的增长,WLST 增加,其中绝大多数是由于脑损伤。超过一半的≥70 岁患者存活下来,这表明不应仅基于年龄将老年多发伤患者排除在积极的损伤治疗之外。