Division of Pediatric Anesthesiology and Critical Care Medicine, Department of Anesthesiology and Critical Care Medicine, Johns Hopkins University School of Medicine, Baltimore, MD.
Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MD.
Crit Care Med. 2020 May;48(5):634-644. doi: 10.1097/CCM.0000000000004291.
With decreasing mortality in PICUs, a growing number of survivors experience long-lasting physical impairments. Early physical rehabilitation and mobilization during critical illness are safe and feasible, but little is known about the prevalence in PICUs. We aimed to evaluate the prevalence of rehabilitation for critically ill children and associated barriers.
National 2-day point prevalence study.
Eighty-two PICUs in 65 hospitals across the United States.
All patients admitted to a participating PICU for greater than or equal to 72 hours on each point prevalence day.
None.
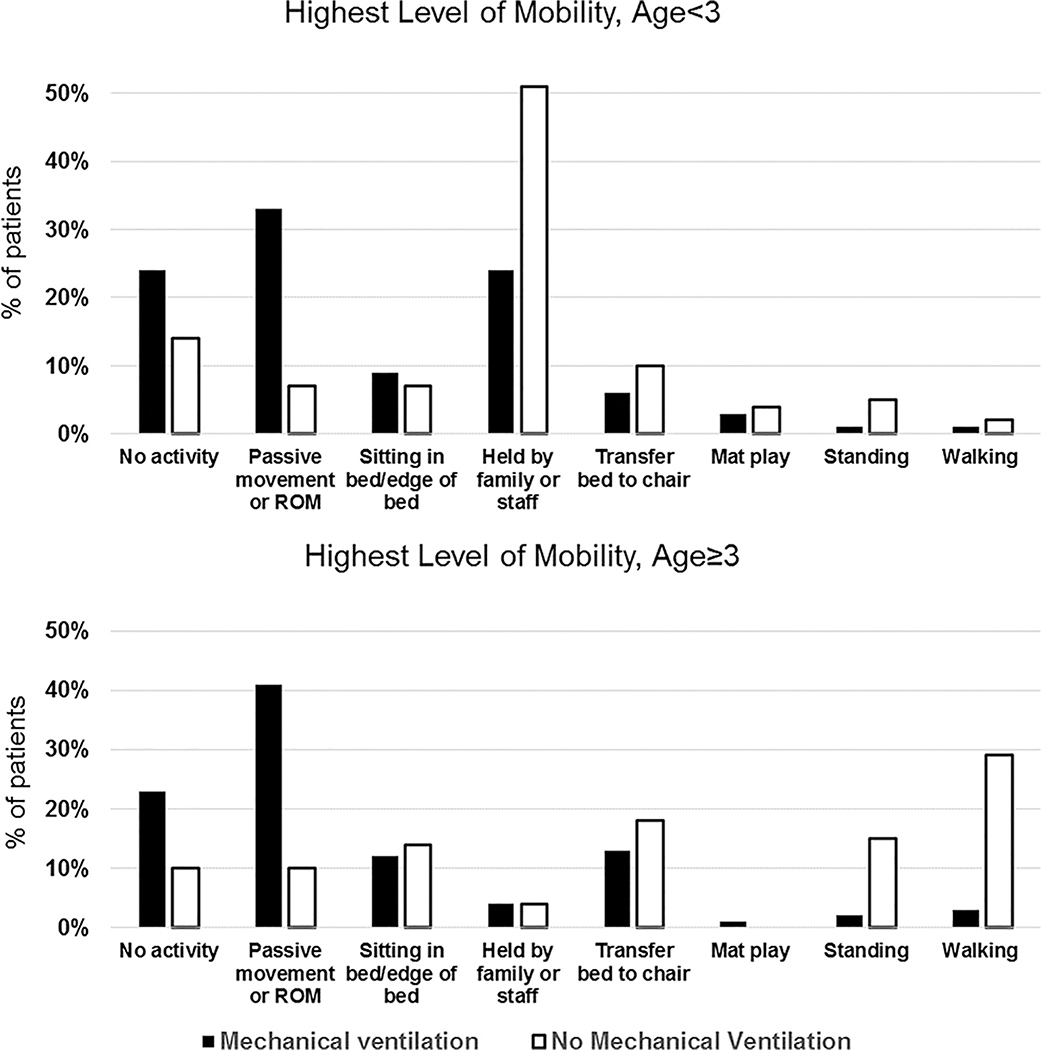
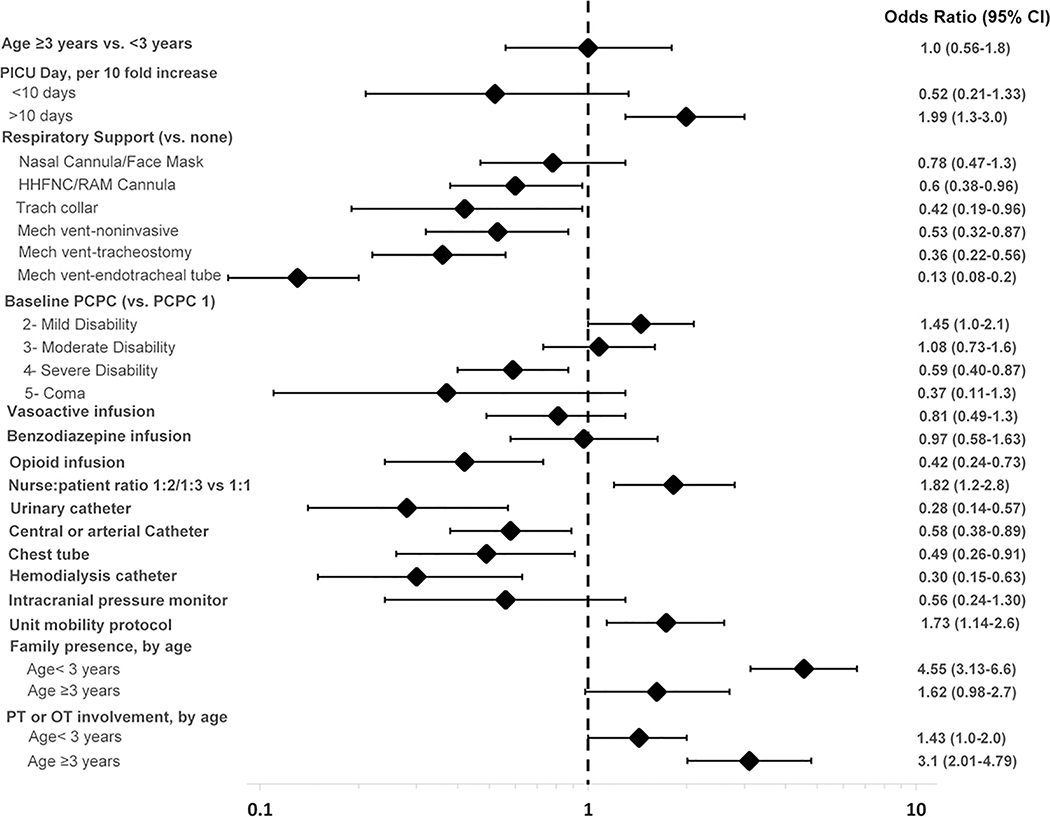
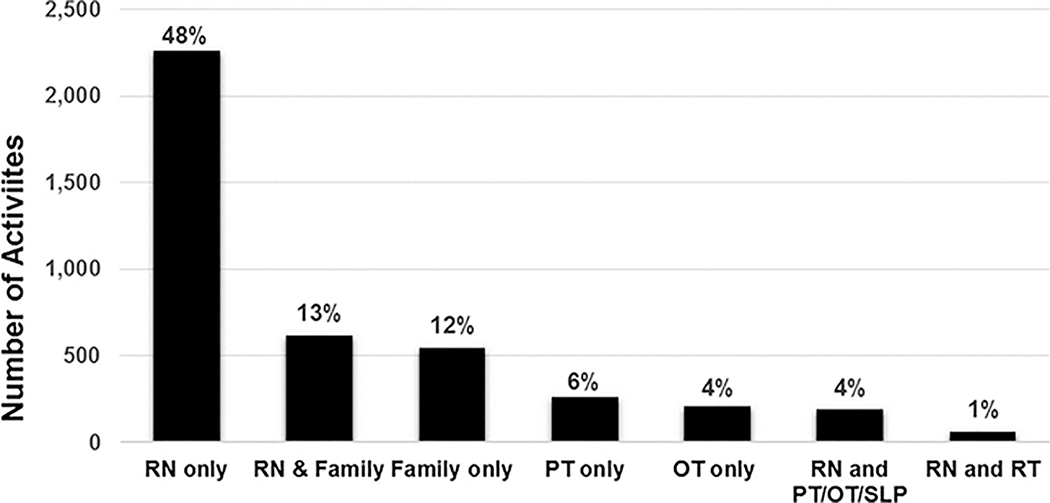
The primary outcome was prevalence of physical therapy- or occupational therapy-provided mobility on the study days. PICUs also prospectively collected timing of initial rehabilitation team consultation, clinical and patient mobility data, potential mobility-associated safety events, and barriers to mobility. The point prevalence of physical therapy- or occupational therapy-provided mobility during 1,769 patient-days was 35% and associated with older age (adjusted odds ratio for 13-17 vs < 3 yr, 2.1; 95% CI, 1.5-3.1) and male gender (adjusted odds ratio for females, 0.76; 95% CI, 0.61-0.95). Patients with higher baseline function (Pediatric Cerebral Performance Category, ≤ 2 vs > 2) less often had rehabilitation consultation within the first 72 hours (27% vs 38%; p < 0.001). Patients were completely immobile on 19% of patient-days. A potential safety event occurred in only 4% of 4,700 mobility sessions, most commonly a transient change in vital signs. Out-of-bed mobility was negatively associated with the presence of an endotracheal tube (adjusted odds ratio, 0.13; 95% CI, 0.1-0.2) and urinary catheter (adjusted odds ratio, 0.28; 95% CI, 0.1-0.6). Positive associations included family presence in children less than 3 years old (adjusted odds ratio, 4.55; 95% CI, 3.1-6.6).
Younger children, females, and patients with higher baseline function less commonly receive rehabilitation in U.S. PICUs, and early rehabilitation consultation is infrequent. These findings highlight the need for systematic design of rehabilitation interventions for all critically ill children at risk of functional impairments.
随着儿科重症监护病房(PICU)死亡率的下降,越来越多的幸存者出现长期的身体功能障碍。在危重病期间早期进行身体康复和活动是安全且可行的,但在 PICU 中,其普及程度尚不清楚。我们旨在评估危重症儿童进行康复治疗的比例,并探讨相关障碍。
全国范围的 2 天时点患病率研究。
美国 65 家医院的 82 个 PICU。
在每个时点患病率日,入住参与研究的 PICU 且大于或等于 72 小时的所有患者。
无。
主要结局为研究日期间接受物理治疗或职业治疗的患者活动能力的患病率。PICU 还前瞻性收集了康复团队首次咨询的时间、临床和患者活动能力数据、潜在与活动相关的安全事件以及活动受限的障碍。在 1769 个患者日中,接受物理治疗或职业治疗的患者活动能力的时点患病率为 35%,与年龄较大(13-17 岁与 < 3 岁相比,调整后的优势比为 2.1;95%置信区间,1.5-3.1)和男性(女性相比,调整后的优势比为 0.76;95%置信区间,0.61-0.95)相关。基线功能(Pediatric Cerebral Performance Category,≤ 2 与 > 2)更高的患者,在最初 72 小时内接受康复咨询的可能性更低(27%与 38%;p < 0.001)。在 19%的患者日中,患者完全无法活动。只有 4%的 4700 次活动中发生潜在的安全事件,最常见的是生命体征的短暂变化。离床活动与气管内插管(调整后的优势比,0.13;95%置信区间,0.1-0.2)和导尿管(调整后的优势比,0.28;95%置信区间,0.1-0.6)的存在呈负相关。阳性关联包括 3 岁以下儿童的家属在场(调整后的优势比,4.55;95%置信区间,3.1-6.6)。
在美国 PICU 中,年龄较小的儿童、女性和基线功能较高的患者较少接受康复治疗,且早期康复咨询的频率较低。这些发现突显了为所有有功能障碍风险的危重症儿童系统设计康复干预措施的必要性。