Department of Pulmonary and Critical Care Medicine, Center of Respiratory Medicine, National Clinical Research Center for Respiratory Diseases, Institute of Respiratory Medicine, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, China.
Department of Tuberculosis and Respiratory Disease, Jinyintan Hospital, Wuhan, China.
Lancet. 2020 Mar 28;395(10229):1054-1062. doi: 10.1016/S0140-6736(20)30566-3. Epub 2020 Mar 11.
Since December, 2019, Wuhan, China, has experienced an outbreak of coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Epidemiological and clinical characteristics of patients with COVID-19 have been reported but risk factors for mortality and a detailed clinical course of illness, including viral shedding, have not been well described.
In this retrospective, multicentre cohort study, we included all adult inpatients (≥18 years old) with laboratory-confirmed COVID-19 from Jinyintan Hospital and Wuhan Pulmonary Hospital (Wuhan, China) who had been discharged or had died by Jan 31, 2020. Demographic, clinical, treatment, and laboratory data, including serial samples for viral RNA detection, were extracted from electronic medical records and compared between survivors and non-survivors. We used univariable and multivariable logistic regression methods to explore the risk factors associated with in-hospital death.
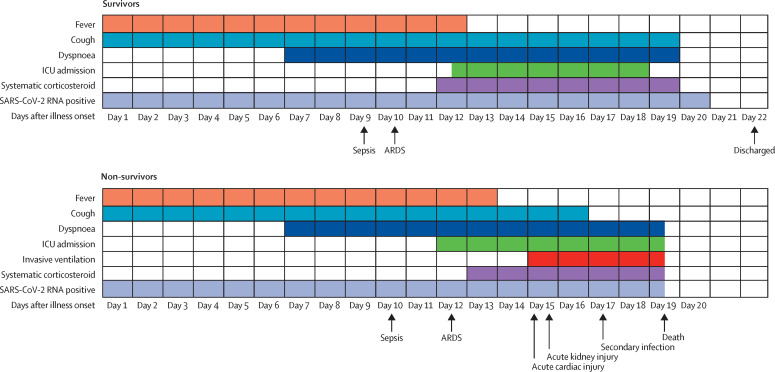
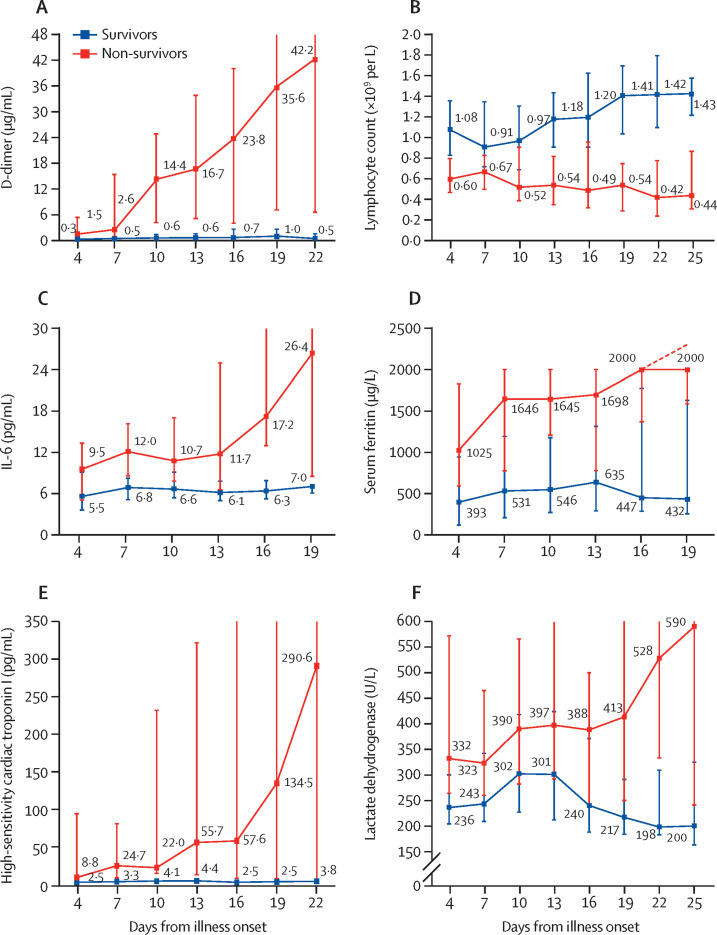
191 patients (135 from Jinyintan Hospital and 56 from Wuhan Pulmonary Hospital) were included in this study, of whom 137 were discharged and 54 died in hospital. 91 (48%) patients had a comorbidity, with hypertension being the most common (58 [30%] patients), followed by diabetes (36 [19%] patients) and coronary heart disease (15 [8%] patients). Multivariable regression showed increasing odds of in-hospital death associated with older age (odds ratio 1·10, 95% CI 1·03-1·17, per year increase; p=0·0043), higher Sequential Organ Failure Assessment (SOFA) score (5·65, 2·61-12·23; p<0·0001), and d-dimer greater than 1 μg/mL (18·42, 2·64-128·55; p=0·0033) on admission. Median duration of viral shedding was 20·0 days (IQR 17·0-24·0) in survivors, but SARS-CoV-2 was detectable until death in non-survivors. The longest observed duration of viral shedding in survivors was 37 days.
The potential risk factors of older age, high SOFA score, and d-dimer greater than 1 μg/mL could help clinicians to identify patients with poor prognosis at an early stage. Prolonged viral shedding provides the rationale for a strategy of isolation of infected patients and optimal antiviral interventions in the future.
Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences; National Science Grant for Distinguished Young Scholars; National Key Research and Development Program of China; The Beijing Science and Technology Project; and Major Projects of National Science and Technology on New Drug Creation and Development.
自 2019 年 12 月以来,中国武汉发生了由严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)引起的 2019 年冠状病毒病(COVID-19)疫情。已经报道了 COVID-19 患者的流行病学和临床特征,但死亡率的危险因素以及详细的临床病程,包括病毒脱落,尚未得到很好的描述。
在这项回顾性的多中心队列研究中,我们纳入了 2020 年 1 月 31 日从金银潭医院和武汉肺科医院出院或死亡的所有经实验室确诊的 COVID-19 成年住院患者(≥18 岁)。从电子病历中提取人口统计学、临床、治疗和实验室数据,包括用于病毒 RNA 检测的连续样本,并在幸存者和非幸存者之间进行比较。我们使用单变量和多变量逻辑回归方法来探讨与院内死亡相关的危险因素。
本研究共纳入 191 例患者(135 例来自金银潭医院,56 例来自武汉肺科医院),其中 137 例出院,54 例院内死亡。91 例(48%)患者有合并症,最常见的是高血压(58 [30%]例),其次是糖尿病(36 [19%]例)和冠心病(15 [8%]例)。多变量回归显示,年龄较大(每增加 1 岁,比值比 1.10,95%置信区间 1.03-1.17;p=0.0043)、序贯器官衰竭评估(SOFA)评分较高(5.65,2.61-12.23;p<0.0001)和入院时 D-二聚体大于 1 μg/mL(18.42,2.64-128.55;p=0.0033)与院内死亡的几率增加相关。幸存者的病毒脱落中位持续时间为 20.0 天(IQR 17.0-24.0),但非幸存者的 SARS-CoV-2 可检测到死亡。在幸存者中最长观察到的病毒脱落时间为 37 天。
年龄较大、SOFA 评分较高和 D-二聚体大于 1 μg/mL 等潜在危险因素有助于临床医生在早期识别预后不良的患者。延长的病毒脱落时间为将来感染患者的隔离和最佳抗病毒干预提供了依据。
中国医学科学院医学与健康科技创新工程基金;国家杰出青年科学基金;国家重点研发计划;北京市科学技术项目;国家新药创制重大科技专项。