Centre de Recherche en Epidémiologie, Biostatistiques et Recherche Clinique, Ecole de Santé Publique, Université Libre de Bruxelles, 1070 Brussels, Belgium.
Institut de Recherche Santé et Sociétés, Faculté de Santé Publique, Université catholique de Louvain, 1200 Brussels, Belgium.
Int J Environ Res Public Health. 2020 Mar 12;17(6):1840. doi: 10.3390/ijerph17061840.
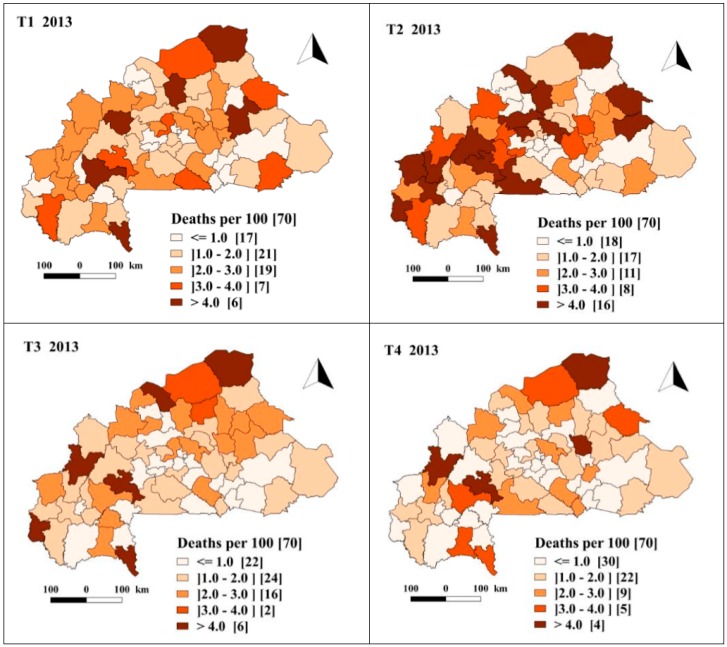
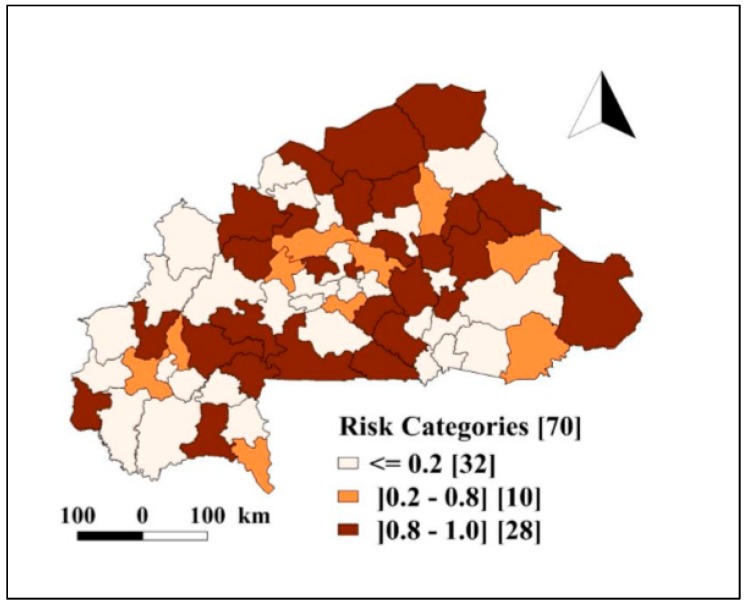
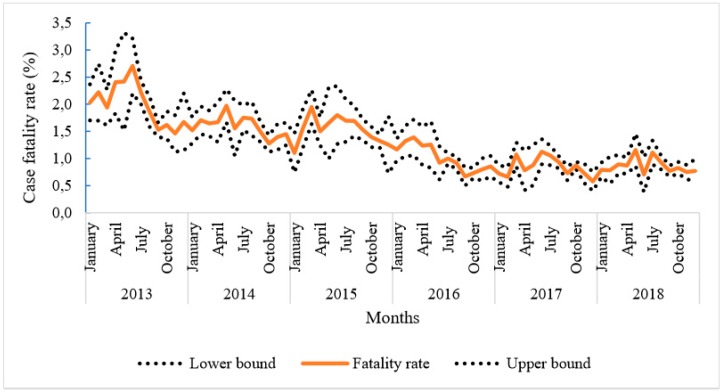
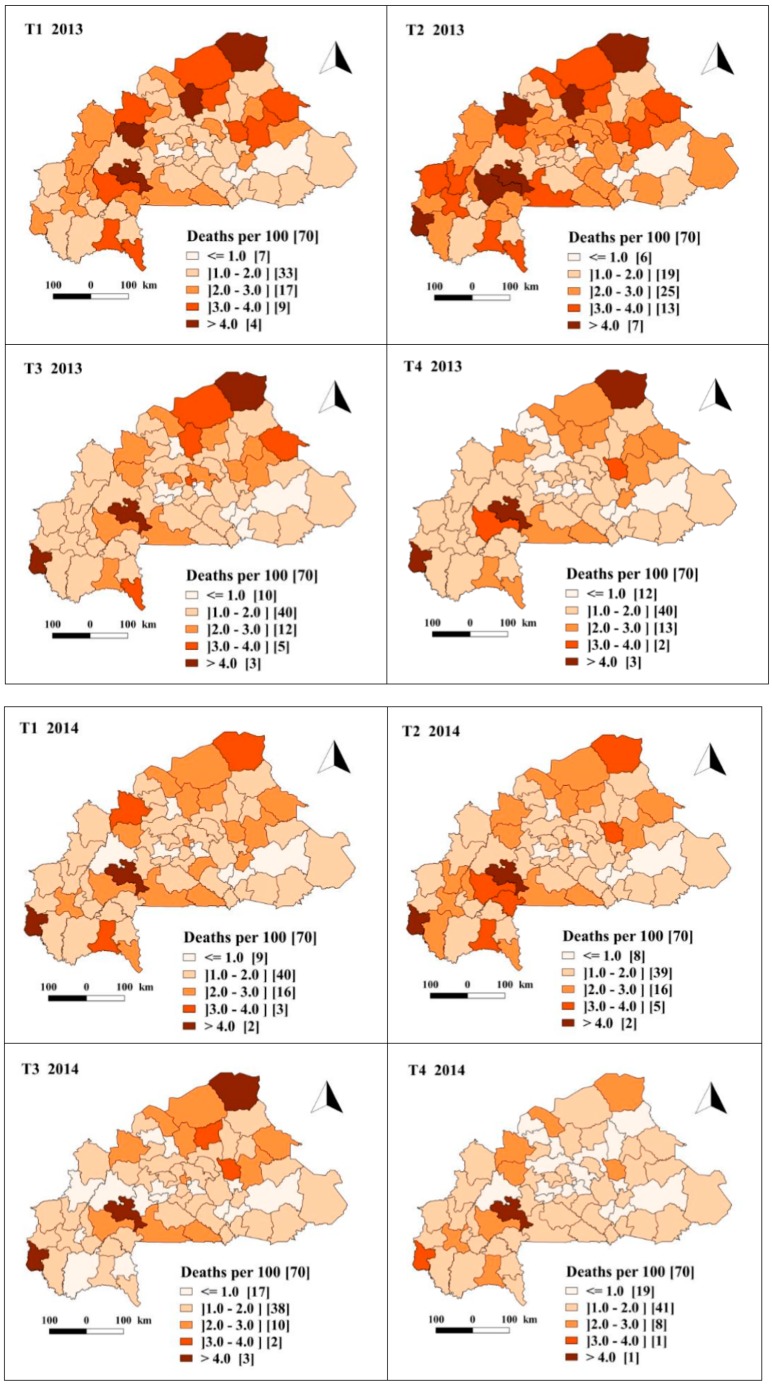
Reducing the 2015 level of malaria mortality by 90% by 2030 is a goal set by the World Health Organization (WHO). In Burkina Faso, several malaria control programs proven to be effective were implemented over the last decade. In parallel, the progressive strengthening of the health surveillance system is generating valuable data, which represents a great opportunity for analyzing the trends in malaria burden and assessing the effect of these control programs. Complementary programs were rolled out at different time points and paces, and the present work aims at investigating both the spatial and temporal pattern of malaria case fatality rate (mCFR) by considering the effect of combining specific and unspecific malaria control programs. To this end, data on severe malaria cases and malaria deaths, aggregated at health district level between January 2013 and December 2018, were extracted from the national health data repository (ENDOS-BF). A Bayesian spatiotemporal zero-inflated Poisson model was fitted to quantify the strength of the association of malaria control programs with monthly mCFR trends at health district level. The model was adjusted for contextual variables. We found that monthly mCFR decreased from 2.0 (95% IC 1.9-2.1%) to 0.9 (95% IC 0.8-1.0%) deaths for 100 severe malaria cases in 2013 and 2018, respectively. Health districts with high mCFR were identified in the northern, northwestern and southwestern parts of the country. The availability of malaria rapid diagnosis tests (IRR: 0.54; CrI: 0.47, 0.62) and treatment (IRR: 0.50; CrI: 0.41, 0.61) were significantly associated with a reduction in the mCFR. The risk of dying from malaria was lower in the period after the free healthcare policy compared with the period before (IRR: 0.47; CrI: 0.38, 0.58). Our findings highlighted locations that are most in need of targeted interventions and the necessity to sustain and strengthen the launched health programs to further reduce the malaria deaths in Burkina Faso.
到 2030 年将疟疾死亡率在 2015 年的基础上降低 90%,这是世界卫生组织(WHO)设定的目标。在布基纳法索,过去十年实施了几项已被证明有效的疟疾控制计划。与此同时,卫生监测系统的逐步加强正在生成有价值的数据,这为分析疟疾负担的趋势和评估这些控制计划的效果提供了绝佳的机会。补充计划在不同的时间点和节奏上展开,本研究旨在通过考虑结合特异性和非特异性疟疾控制计划的效果,调查疟疾病死率(mCFR)的时空模式。为此,从国家卫生数据存储库(ENDOS-BF)中提取了 2013 年 1 月至 2018 年 12 月期间按卫生区汇总的重症疟疾病例和疟疾死亡病例的数据。拟合了贝叶斯时空零膨胀泊松模型来量化疟疾控制计划与卫生区水平的每月 mCFR 趋势之间的关联强度。该模型针对背景变量进行了调整。我们发现,与 2013 年相比,2018 年每月 mCFR 从每 100 例重症疟疾死亡 2.0(95%CI 1.9-2.1%)下降至 0.9(95%CI 0.8-1.0%)。在该国北部、西北部和西南部发现了 mCFR 较高的卫生区。疟疾快速诊断检测(IRR:0.54;CrI:0.47,0.62)和治疗(IRR:0.50;CrI:0.41,0.61)的可及性与 mCFR 的降低显著相关。与免费医疗政策实施前相比,实施免费医疗政策后疟疾死亡的风险更低(IRR:0.47;CrI:0.38,0.58)。我们的研究结果突出了最需要有针对性干预的地点,并需要维持和加强已启动的卫生计划,以进一步减少布基纳法索的疟疾死亡人数。