Sorbets Emmanuel, Steg Philippe Gabriel
Hôtel-Dieu, Assistance Publique - Hôpitaux de Paris, Université de Paris, Paris, France.
Royal Brompton Hospital, National Heart and Lung Institute, Imperial College, London, UK.
Eur Cardiol. 2020 Feb 26;15:1-7. doi: 10.15420/ecr.2018.24.2. eCollection 2020 Feb.
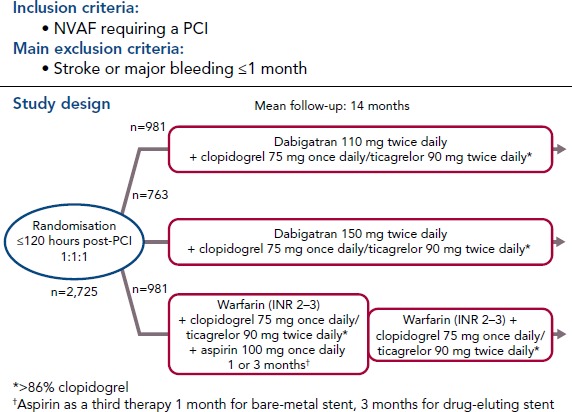
Direct-acting oral anticoagulants (DOACs) are easier to use, safer than and as effective as vitamin K antagonists (VKA) in the treatment of non-valvular AF (NVAF). Because of their favourable safety profile and easier use than VKAs, DOACs as anti-thrombotic therapy may have a role in the management of chronic coronary syndromes (CCS). To date, few studies have evaluated DOACs in this setting. Initial studies have focused on patients receiving DOACs for NVAF undergoing acute or elective percutaneous coronary intervention who additionally require dual antiplatelet therapy (DAPT). Rivaroxaban 15 mg once daily plus a P2Y inhibitor compared with a VKA regimen was associated with a reduction of bleedings (HR 0.59; 95% CI [0.47-0.76]; p<0.001). Rivaroxaban 2.5 mg twice daily plus DAPT up to 12 months followed by rivaroxaban 15 mg once daily plus P2Y inhibitor showed similar results. Dabigatran 110 mg twice daily plus a P2Y inhibitor versus a VKA regimen was associated with a reduction of bleedings (HR 0.52; 95% CI [0.42-0.63]; p<0.001), after a mean follow-up of 14 months. A dabigatran 150 mg regimen showed similar results. Apixaban 5 mg twice daily plus a P2Y inhibitor versus a VKA regimen confirmed at 6 months the safety of DOACs with a reduction of bleedings (HR 0.69; 95% CI [0.58-0.81]; p<0.001 for non-inferiority and superiority). Edoxaban 60 mg once daily plus a P2Y inhibitor was non-inferior to a VKA regimen on bleeding outcomes (major bleeding or non-major clinically relevant non-major bleeding) after a 12-month follow-up (HR 0.83; 95% CI [0.65-1.05]; p=0.001 for non-inferiority; p=0.1154 for superiority). Meta-analysis of these four trials confirmed the safety of DOACs regarding bleeding outcomes, but showed a trend toward stent thrombosis for dual antithrombotic therapy using DOACs versus triple antithrombotic therapy using VKAs. DOACs may show promise in the management of high-risk patients with chronic coronary syndromes. In these patients, rivaroxaban 2.5 mg twice daily in addition to aspirin was shown to reduce the composite outcome of cardiovascular death, stroke or MI compared to aspirin alone (HR 0.76; 95% CI [0.66-0.86]; p<0.001). All-cause death, cardiovascular death and stroke were also significantly lower. This benefit was at the cost of an increase in non-fatal bleeding.
直接口服抗凝剂(DOACs)使用更便捷,在治疗非瓣膜性房颤(NVAF)方面比维生素K拮抗剂(VKA)更安全且疗效相当。由于其良好的安全性以及比VKA更易于使用,DOACs作为抗血栓治疗可能在慢性冠状动脉综合征(CCS)的管理中发挥作用。迄今为止,很少有研究评估DOACs在这种情况下的效果。初步研究集中在接受DOACs治疗NVAF且需要接受急性或择期经皮冠状动脉介入治疗并额外需要双重抗血小板治疗(DAPT)的患者。与VKA方案相比,每日一次服用15 mg利伐沙班加一种P2Y抑制剂与出血减少相关(风险比0.59;95%置信区间[0.47 - 0.76];p<0.001)。每日两次服用2.5 mg利伐沙班加DAPT持续12个月,随后每日一次服用15 mg利伐沙班加P2Y抑制剂显示出相似结果。与VKA方案相比,每日两次服用110 mg达比加群加一种P2Y抑制剂在平均随访14个月后与出血减少相关(风险比0.52;95%置信区间[0.42 - 0.63];p<0.001)。150 mg达比加群方案显示出相似结果。与VKA方案相比,每日两次服用5 mg阿哌沙班加一种P2Y抑制剂在6个月时证实了DOACs的安全性,出血减少(风险比0.69;95%置信区间[0.58 - 0.81];非劣效性和优效性p<0.001)。在12个月随访后,每日一次服用60 mg依度沙班加一种P2Y抑制剂在出血结局(大出血或非大出血但具有临床相关性)方面不劣于VKA方案(风险比0.83;95%置信区间[0.65 - 1.05];非劣效性p = 0.001;优效性p = 0.1154)。对这四项试验的荟萃分析证实了DOACs在出血结局方面的安全性,但显示出与使用VKA的三联抗血栓治疗相比,使用DOACs的双重抗血栓治疗有支架血栓形成的趋势。DOACs在慢性冠状动脉综合征高危患者的管理中可能显示出前景。在这些患者中,与单独使用阿司匹林相比,除阿司匹林外每日两次服用2.5 mg利伐沙班可降低心血管死亡、中风或心肌梗死的复合结局(风险比0.76;95%置信区间[0.66 - 0.86];p<0.001)。全因死亡、心血管死亡和中风也显著降低。这种益处是以非致命性出血增加为代价的。