Liang Bo, Zhu Yong-Chun, Gu Ning
Nanjing University of Chinese Medicine, Nanjing, China.
Nanjing Hospital of Chinese Medicine Affiliated to Nanjing University of Chinese Medicine, Nanjing, China.
Front Cardiovasc Med. 2022 Mar 21;9:832164. doi: 10.3389/fcvm.2022.832164. eCollection 2022.
Antithrombotic therapy for patients with atrial fibrillation undergoing percutaneous coronary intervention is facing major treatment problems in clinical practice.
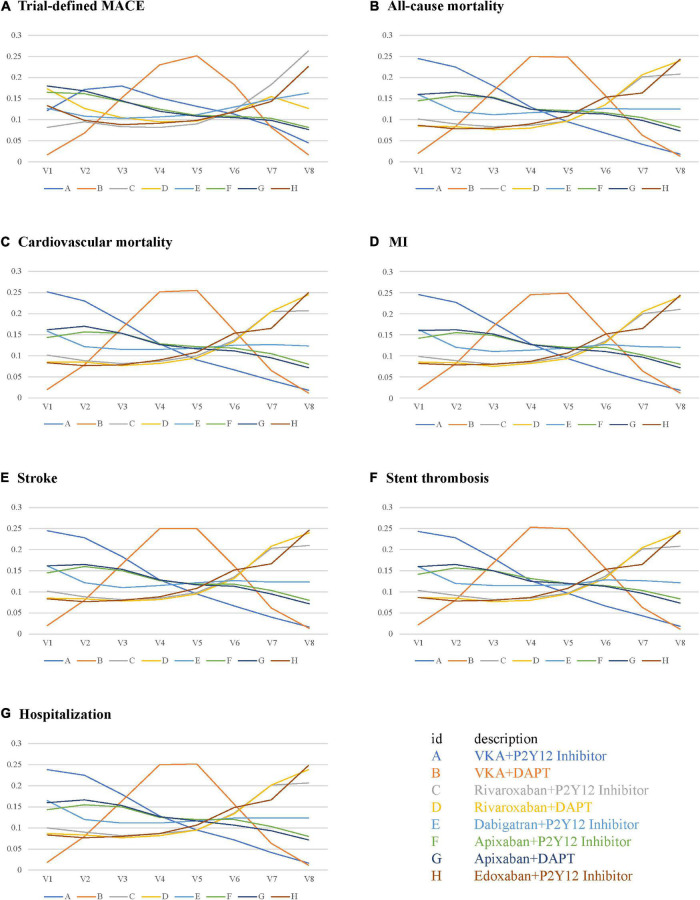
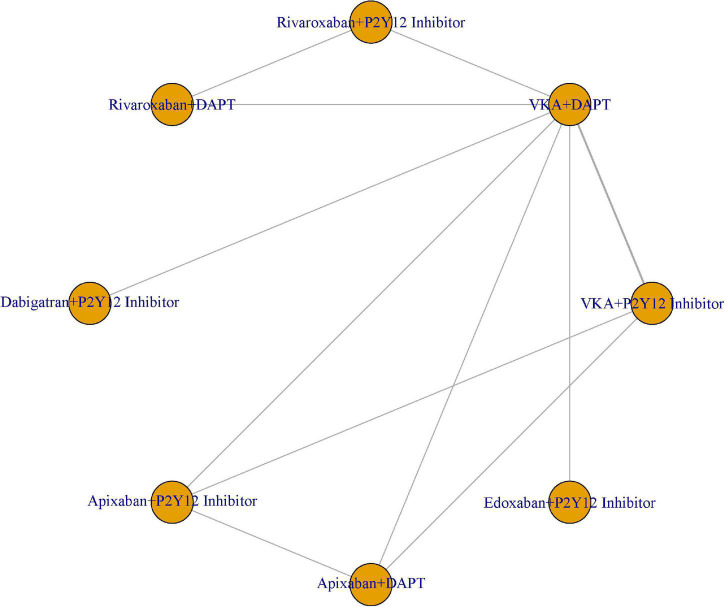
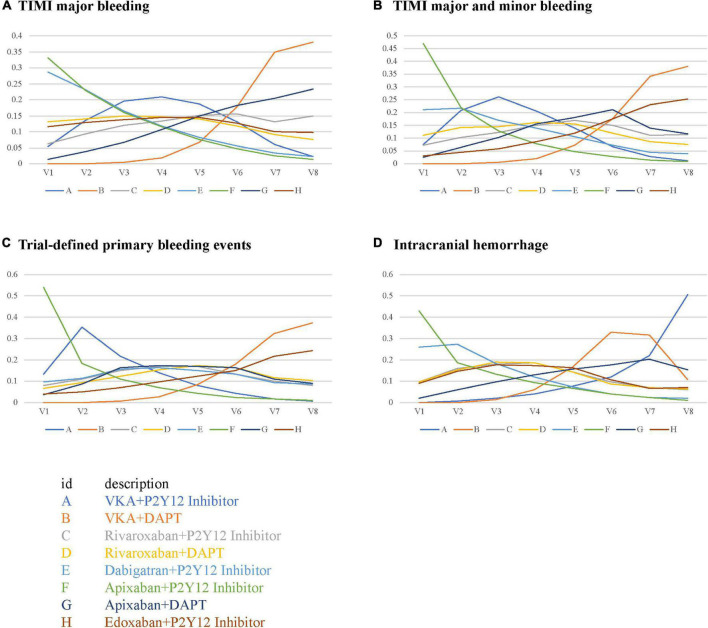
We firstly conducted a Bayesian network meta-analysis to study the safety and efficacy of different antithrombotic regimens. Only randomized controlled trials from PubMed, Web of Science, Cochrane Central Register of Controlled Trials, Embase, and China National Knowledge Infrastructure were included in our study. The Bayesian random-effects model was used in this study. The primary safety and efficacy outcomes were major bleeding according to the criteria of Thrombolysis In Myocardial Infarction (TIMI) and trial-defined major adverse cardiovascular events, respectively. The secondary safety outcomes were combined TIMI major and minor bleeding, trial-defined primary bleeding events, and intracranial hemorrhage. The secondary efficacy outcomes were all-cause or cardiovascular mortality, myocardial infarction, stroke, stent thrombosis, and hospitalization.
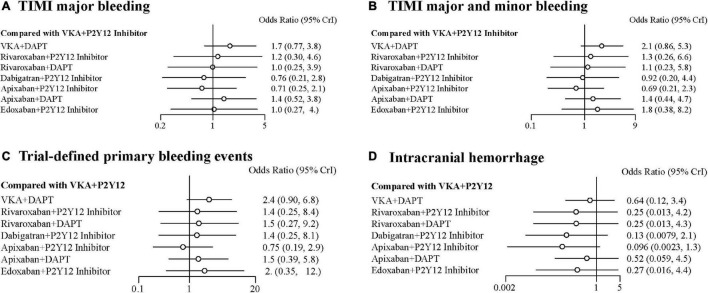
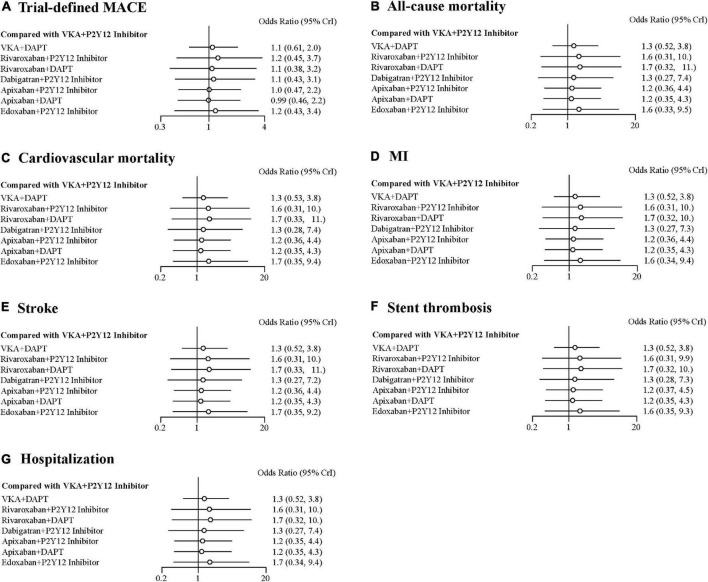
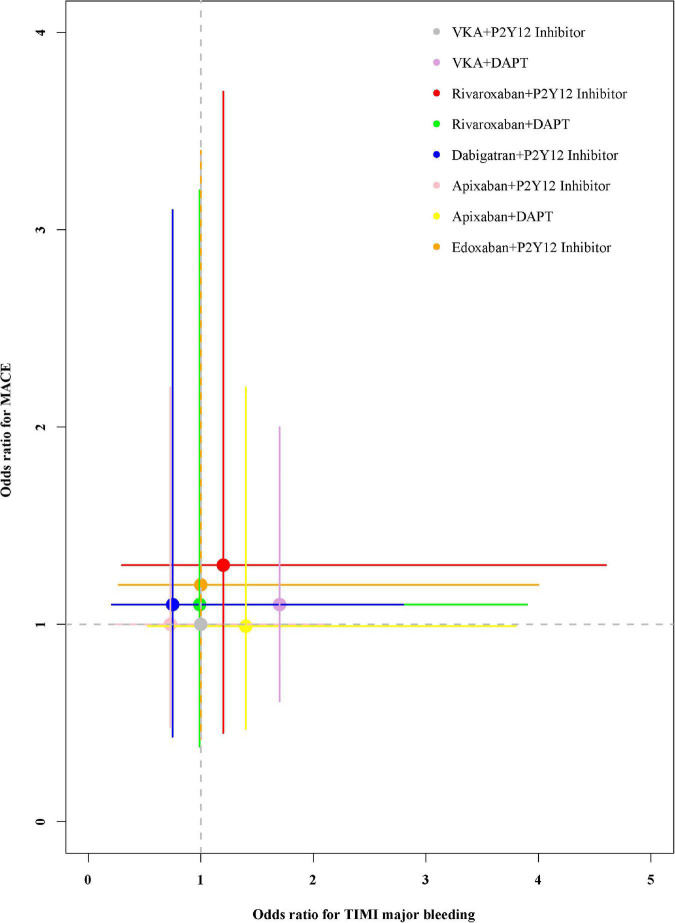
Total of 11,532 patients from the five randomized controlled trials were analyzed, of whom 8,426 were male. Compared with vitamin K antagonist (VKA) plus P2Y12 inhibitor, the odds ratios (95% credible intervals) for TIMI major bleeding were 1.70 (0.77-3.80) for VKA plus dual antiplatelet therapy (DAPT), 1.20 (0.30-4.60) for rivaroxaban plus P2Y12 inhibitor, 1.00 (0.25-3.90) for rivaroxaban plus DAPT, 0.76 (0.21-2.80) for dabigatran plus P2Y12 inhibitor, 0.71 (0.25-2.10) for apixaban plus P2Y12 inhibitor, 1.40 (0.52-3.80) for apixaban plus DAPT, and 1.00 (0.27-4.00) for edoxaban plus P2Y12 inhibitor. For trial-defined major adverse cardiovascular events, compared with VKA plus P2Y12 inhibitor, the odds ratios (95% credible intervals) were 1.10 (0.61-2.00) for VKA plus DAPT, 1.20 (0.45-3.70) for rivaroxaban plus P2Y12 inhibitor, 1.10 (0.38-3.20) for rivaroxaban plus DAPT, 1.10 (0.43-3.10) for dabigatran plus P2Y12 inhibitor, 1.00 (0.47-2.20) for apixaban plus P2Y12 inhibitor, 0.99 (0.46-2.20) for apixaban plus DAPT, and 1.20 (0.43-3.40) for edoxaban plus P2Y12 inhibitor. Apixaban plus P2Y12 inhibitor was the highest-ranking of safety outcomes and VKA plus P2Y12 inhibitor was the highest-ranking of efficacy outcomes other than trial-defined major adverse cardiovascular events.
Apixaban plus P2Y12 inhibitor seems to be linked with fewer bleeding complications while retaining antithrombotic efficacy. Moreover, for most efficacy indicators, the ranking of VKA plus P2Y12 inhibitor is still very high.
[www.crd.york.ac.uk/prospero/], identifier [CRD42020149894].
接受经皮冠状动脉介入治疗的心房颤动患者的抗栓治疗在临床实践中面临重大治疗问题。
我们首先进行了一项贝叶斯网络荟萃分析,以研究不同抗栓方案的安全性和有效性。本研究仅纳入了来自PubMed、科学网、Cochrane对照试验中央注册库、Embase和中国知网的随机对照试验。本研究采用贝叶斯随机效应模型。主要安全性和有效性结局分别为根据心肌梗死溶栓(TIMI)标准定义的大出血和试验定义的主要不良心血管事件。次要安全性结局为TIMI大出血和小出血合并、试验定义的主要出血事件和颅内出血。次要有效性结局为全因或心血管死亡率、心肌梗死、中风、支架血栓形成和住院治疗。
分析了五项随机对照试验中的11532例患者,其中8426例为男性。与维生素K拮抗剂(VKA)加P2Y12抑制剂相比,VKA加双联抗血小板治疗(DAPT)的TIMI大出血比值比(95%可信区间)为1.70(0.77 - 3.80),利伐沙班加P2Y12抑制剂为1.20(0.30 - 4.60),利伐沙班加DAPT为1.00(0.25 - 3.90),达比加群加P2Y12抑制剂为0.76(0.21 - 2.80),阿哌沙班加P2Y12抑制剂为0.71(0.25 - 2.10),阿哌沙班加DAPT为1.40(0.52 - 3.80),依度沙班加P2Y12抑制剂为1.00(0.27 - 4.00)。对于试验定义的主要不良心血管事件,与VKA加P2Y12抑制剂相比,VKA加DAPT的比值比(95%可信区间)为1.10(0.61 - 2.00),利伐沙班加P2Y12抑制剂为1.20(0.45 - 3.70),利伐沙班加DAPT为1.10(0.38 - 3.20),达比加群加P2Y12抑制剂为1.10(0.43 - 3.10),阿哌沙班加P2Y12抑制剂为1.00(0.47 - 2.20),阿哌沙班加DAPT为0.99(0.46 - 2.20),依度沙班加P2Y12抑制剂为1.20(0.43 - 3.40)。阿哌沙班加P2Y12抑制剂在安全性结局中排名最高,而VKA加P2Y12抑制剂在除试验定义的主要不良心血管事件外的有效性结局中排名最高。
阿哌沙班加P2Y12抑制剂似乎与较少的出血并发症相关,同时保持抗栓疗效。此外,对于大多数有效性指标,VKA加P2Y12抑制剂的排名仍然很高。