Abravan Azadeh, Eide Hanne Astrid, Helland Åslaug, Malinen Eirik
Department of Medical Physics, Oslo University Hospital, Oslo, Norway.
Department of Physics, University of Oslo, Oslo, Norway.
Clin Transl Radiat Oncol. 2020 Feb 19;22:15-21. doi: 10.1016/j.ctro.2020.02.005. eCollection 2020 May.
Lymphopenia during radiotherapy (RT) may have an adverse effect on treatment outcome. The aim of this study is to investigate associations between lymphopenia and RT parameters in patients with advanced lung cancer. Moreover, to investigate the prognostic role of lymphopenia, blood protein levels, and treatment and patient-related factors.
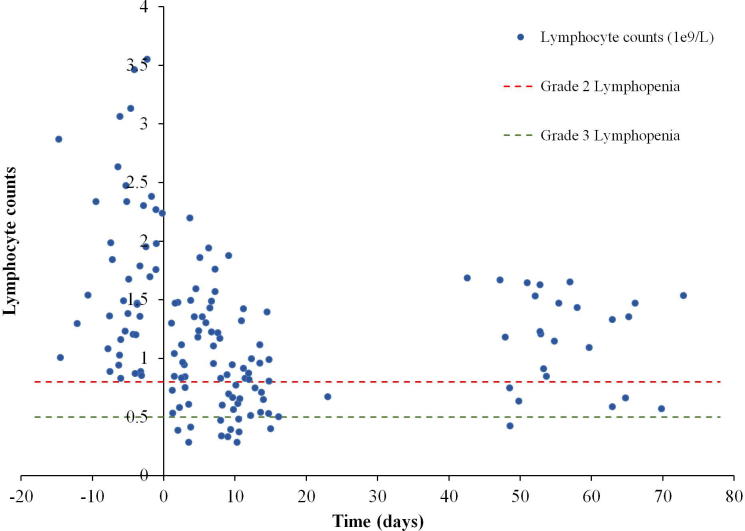
Sixty-two advanced stage non-small cell lung cancer (NSCLC) patients were retrospectively analyzed. Blood counts were available prior to, during, and after RT (3Gyx10). For each patient, a thoracic volume of interest (VOI) -including thoracic soft tissue and trabecular bone- was obtained by applying a CT window of -500 to 1200 HU in the planning CT. Dose parameters from thoracic VOI and other regions including lungs and vertebrae were calculated. Association between risk of lymphopenia ≥ G3 (lymphocytes at nadir according to CTCAE v4.0) and therapeutic parameters was investigated using Logistic regression. Relationships between overall survival (OS) and RT dose parameters, baseline blood counts and protein levels, and clinical factors were evaluated using Log-rank and Cox models.
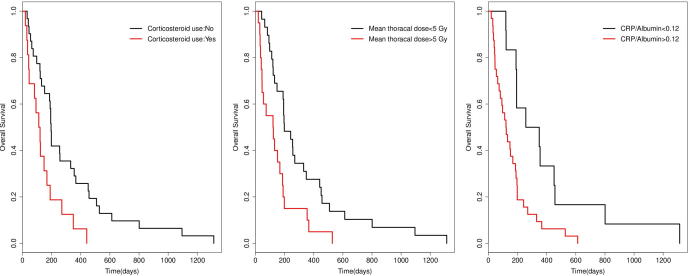
Mean thoracic RT dose (odds ratio [OR] 1.67; p = 0.04), baseline lymphocytes (OR 0.65; p = 0.01), and corticosteroids use (OR 6.07; p = 0.02) were significantly associated with increased risk of lymphopenia ≥ G3 in multivariable analysis. Worse OS was associated with high mean thoracic RT dose, high CRP/Albumin, large tumor volume and corticosteroids use (p < 0.05, univariate analysis), but not with lymphopenia ≥ G3. CRP/Albumin ratio > 0.12 (hazard ratio [HR] 2.28, p = 0.03) and corticosteroid use (HR 2.52, p = 0.01) were independently associated with worse OS.
High thoracic RT dose gave a higher risk of lymphopenia ≥ G3; hence limiting dose volume to the thorax may be valuable in preventing severe lymphopenia for patients receiving palliative fractionated RT. Still, lymphopenia ≥ G3 was not associated with worse OS. however, high baseline CRP/Albumin was associated with poorer OS and may carry important information as a prognostic factor of OS in advanced NSCLC receiving palliative RT.
放疗(RT)期间淋巴细胞减少可能对治疗结果产生不利影响。本研究的目的是调查晚期肺癌患者淋巴细胞减少与放疗参数之间的关联。此外,研究淋巴细胞减少、血液蛋白水平以及治疗和患者相关因素的预后作用。
回顾性分析62例晚期非小细胞肺癌(NSCLC)患者。在放疗前、放疗期间和放疗后(3Gyx10)均可获得血常规数据。对于每位患者,通过在计划CT中应用-500至1200HU的CT窗获得包括胸部软组织和小梁骨在内的胸部感兴趣体积(VOI)。计算胸部VOI和包括肺和椎骨在内的其他区域的剂量参数。使用逻辑回归研究淋巴细胞减少≥G3级(根据CTCAE v4.0的最低点淋巴细胞计数)风险与治疗参数之间的关联。使用对数秩检验和Cox模型评估总生存期(OS)与放疗剂量参数、基线血常规和蛋白水平以及临床因素之间的关系。
多变量分析显示,胸部放疗平均剂量(比值比[OR]1.67;p = 0.04)、基线淋巴细胞计数(OR 0.65;p = 0.01)和使用皮质类固醇(OR 6.07;p = 0.02)与淋巴细胞减少≥G3级风险增加显著相关。较差的总生存期与胸部放疗平均剂量高、CRP/白蛋白比值高、肿瘤体积大以及使用皮质类固醇有关(单变量分析,p < 0.05),但与淋巴细胞减少≥G3级无关。CRP/白蛋白比值>0.12(风险比[HR]2.28,p = 0.03)和使用皮质类固醇(HR 2.52,p = 0.01)与较差的总生存期独立相关。
胸部放疗高剂量会使淋巴细胞减少≥G3级的风险更高;因此,对于接受姑息性分割放疗的患者,限制胸部的剂量体积可能对预防严重淋巴细胞减少有价值。尽管如此,淋巴细胞减少≥G3级与较差的总生存期无关。然而,高基线CRP/白蛋白与较差的总生存期相关,并且可能作为接受姑息性放疗的晚期NSCLC患者总生存期的预后因素携带重要信息。