Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Korea.
Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Korea.
J Korean Med Sci. 2020 Mar 23;35(11):e70. doi: 10.3346/jkms.2020.35.e70.
Previously, a linked pharmacokinetic-pharmacodynamic model (the Kim model) of propofol with concurrent infusion of remifentanil was developed for children aged 2-12 years. There are few options for pharmacokinetic-pharmacodynamic model of propofol for children under two years old. We performed an external validation of the Kim model for children under two years old to evaluate whether the model is applicable to this age group.
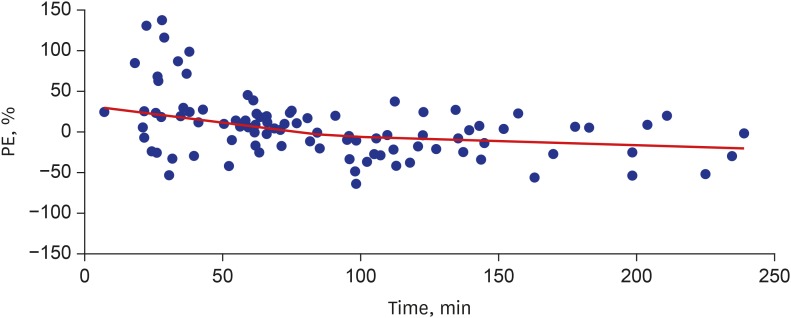
Twenty-four children were enrolled. After routine anesthetic induction, a continuous infusion of 2% propofol and remifentanil was commenced using the Kim model. The target effect-site concentration of propofol was set as 2, 3, 4, and 5 μg/mL, followed by arterial blood sampling after 10 min of each equilibrium. Population estimates of four parameters-pooled bias, inaccuracy, divergence, and wobble-were used to evaluate the performance of the Kim model.
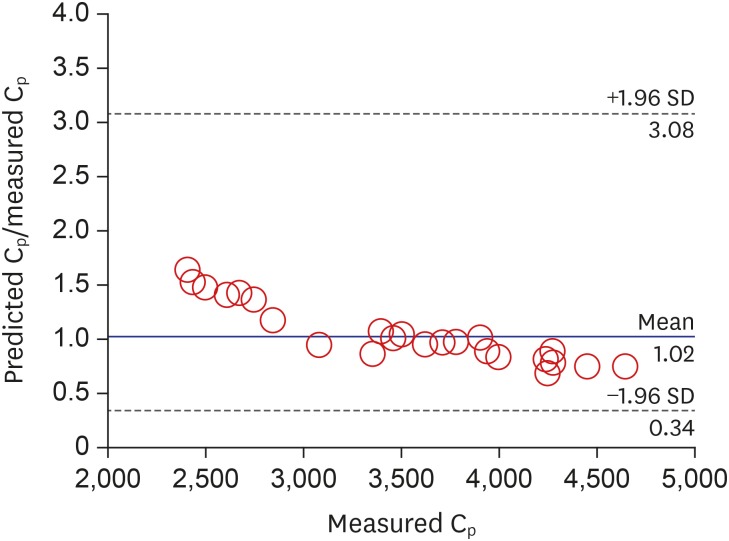
A total of 95 plasma concentrations were used for evaluation of the Kim model. The population estimate (95% confidence interval) of bias was -0.96% (-8.45%, 6.54%) and that of inaccuracy was 21.0% (15.0%-27.0%) for the plasma concentration of propofol.
The pooled bias and inaccuracy of the pharmacokinetic predictions are clinically acceptable. Therefore, our external validation of the Kim model indicated that the model can be applicable to target-controlled infusion of propofol in children younger than 2 years, with the recommended use of actual bispectral index monitoring in clinical settings that remifentanil is present.
Clinical Research Information Service Identifier: KCT0001752.
先前,我们建立了一种包含瑞芬太尼的丙泊酚药代动力学药效学模型(Kim 模型),适用于 2-12 岁儿童。但对于 2 岁以下儿童的丙泊酚药代动力学药效学模型选择较少。因此,我们对 Kim 模型进行了 2 岁以下儿童的外部验证,以评估该模型是否适用于该年龄组。
共纳入 24 名儿童。在常规麻醉诱导后,使用 Kim 模型开始输注 2%丙泊酚和瑞芬太尼。将丙泊酚的目标效应部位浓度设定为 2、3、4 和 5 μg/ml,在每个平衡期后 10 min 进行动脉采血。使用四个参数的群体估计值——综合偏差、不准确性、发散性和晃动性来评估 Kim 模型的性能。
共评估了 95 个丙泊酚血浆浓度以评价 Kim 模型。丙泊酚血浆浓度的群体估计值(95%置信区间)为偏差-0.96%(-8.45%,6.54%),不准确性 21.0%(15.0%-27.0%)。
药代动力学预测的综合偏差和不准确性在临床上是可以接受的。因此,我们对 Kim 模型的外部验证表明,该模型可适用于 2 岁以下儿童丙泊酚靶控输注,建议在存在瑞芬太尼的临床环境中使用实际的脑电双频指数监测。
临床研究信息服务识别码:KCT0001752。