Brodersen John, Voss Theis, Martiny Frederik, Siersma Volkert, Barratt Alexandra, Heleno Bruno
The Section of General Practice and the Research Unit for General Practice, Dept of Public Health, University of Copenhagen, Copenhagen, Denmark.
The Research Unit for General Practice in Region Zealand, Sorø, Denmark.
Breathe (Sheff). 2020 Mar;16(1):200013. doi: 10.1183/20734735.0013-2020.
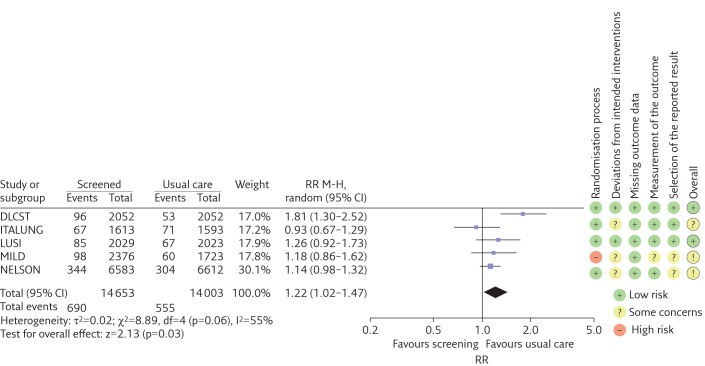
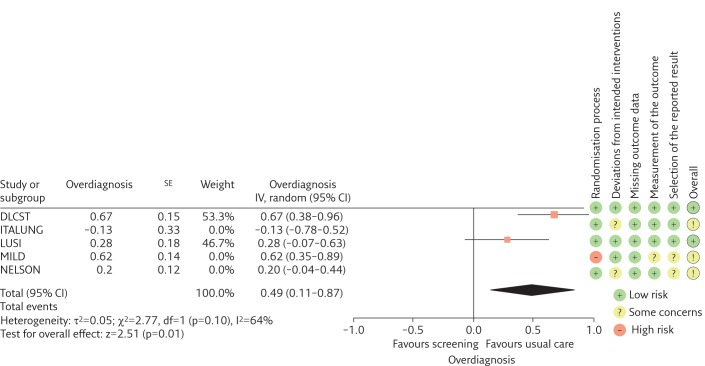
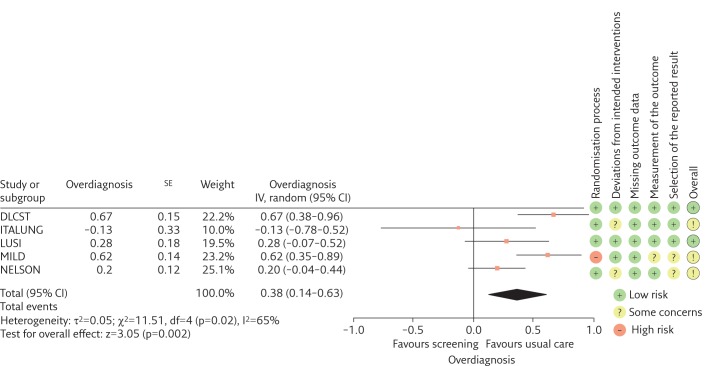
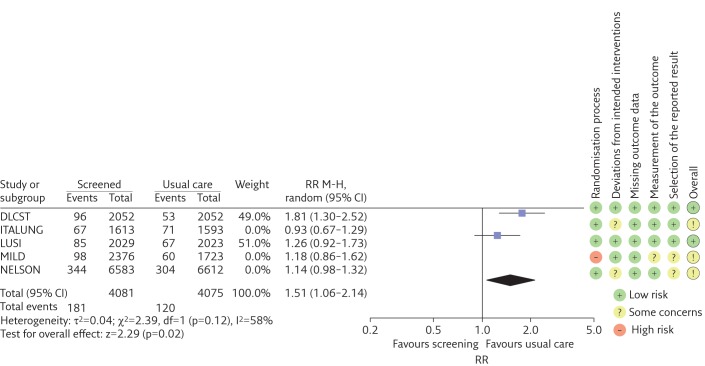
In low-dose computed tomography (LDCT) screening for lung cancer, all three main conditions for overdiagnosis in cancer screening are present: 1) a reservoir of slowly or nongrowing lung cancer exists; 2) LDCT is a high-resolution imaging technology with the potential to identify this reservoir; and 3) eligible screening participants have a high risk of dying from causes other than lung cancer. The degree of overdiagnosis in cancer screening is most validly estimated in high-quality randomised controlled trials (RCTs), with enough follow-up time after the end of screening to avoid lead-time bias and without contamination of the control group. Nine RCTs investigating LDCT screening were identified. Two RCTs were excluded because lung cancer incidence after the end of screening was not published. Two other RCTs using active comparators were also excluded. Therefore, five RCTs were included: two trials were at low risk of bias, two of some concern and one at high risk of bias. In a meta-analysis of the two low risk of bias RCTs including 8156 healthy current or former smokers, 49% of the screen-detected cancers were overdiagnosed. There is uncertainty about this substantial degree of overdiagnosis due to unexplained heterogeneity and low precision of the summed estimate across the two trials.
Nine randomised controlled trials (RCTs) on low-dose computed tomography screening were identified; five were included for meta-analysis but only two of those were at low risk of bias.In a meta-analysis of recent low risk of bias RCTs including 8156 healthy current or former smokers from developed countries, we found that 49% of the screen-detected cancers may be overdiagnosed.There is uncertainty about the degree of overdiagnosis in lung cancer screening due to unexplained heterogeneity and low precision of the point estimate.If only high-quality RCTs are included in the meta-analysis, the degree of overdiagnosis is substantial.
To appreciate that low-dose computed tomography screening for lung cancer meets all three main conditions for overdiagnosis in cancer screening: a reservoir of indolent cancers exists in the population; the screening test is able to "tap" this reservoir by detecting biologically indolent cancers as well as biologically important cancers; and the population being screened is characterised by a relatively high competing risk of death from other causesTo learn about biases that might affect the estimates of overdiagnosis in randomised controlled trials in cancer screening.
在低剂量计算机断层扫描(LDCT)肺癌筛查中,癌症筛查中过度诊断的所有三个主要条件均存在:1)存在缓慢生长或不生长的肺癌储备;2)LDCT是一种高分辨率成像技术,有潜力识别出这种储备;3)符合条件的筛查参与者死于肺癌以外原因的风险很高。癌症筛查中过度诊断的程度在高质量随机对照试验(RCT)中评估最为有效,在筛查结束后要有足够的随访时间以避免领先时间偏倚,且对照组未受污染。共识别出9项研究LDCT筛查的RCT。两项RCT被排除,因为筛查结束后的肺癌发病率未公布。另外两项使用活性对照的RCT也被排除。因此,纳入了5项RCT:两项试验偏倚风险低,两项有些问题,一项偏倚风险高。在对两项偏倚风险低的RCT进行的荟萃分析中,纳入了8156名当前或既往吸烟的健康者,筛查发现的癌症中有49%被过度诊断。由于无法解释的异质性以及两项试验汇总估计的低精度,对于这种相当程度的过度诊断存在不确定性。
识别出9项关于低剂量计算机断层扫描筛查的随机对照试验(RCT);5项纳入荟萃分析,但其中只有两项偏倚风险低。在对近期偏倚风险低的RCT进行的荟萃分析中,纳入了来自发达国家的8156名当前或既往吸烟的健康者,我们发现筛查发现的癌症中有49%可能被过度诊断。由于无法解释的异质性以及点估计的低精度,肺癌筛查中过度诊断的程度存在不确定性。如果荟萃分析仅纳入高质量RCT,过度诊断的程度相当大。
认识到低剂量计算机断层扫描肺癌筛查满足癌症筛查中过度诊断的所有三个主要条件:人群中存在惰性癌症储备;筛查试验能够通过检测生物学上惰性的癌症以及生物学上重要的癌症来“挖掘”这种储备;被筛查人群的特征是死于其他原因的竞争风险相对较高。了解可能影响癌症筛查随机对照试验中过度诊断估计的偏倚。