Lancet Glob Health. 2020 Apr;8(4):e545-e554. doi: 10.1016/S2214-109X(20)30034-6.
We aimed to evaluate and improve the accuracy of the ultrasound scan in estimating gestational age in late pregnancy (ie, after 24 weeks' gestation) in low-income and middle-income countries (LMICs), where access to ultrasound in the first half of pregnancy is rare and where intrauterine growth restriction is prevalent.
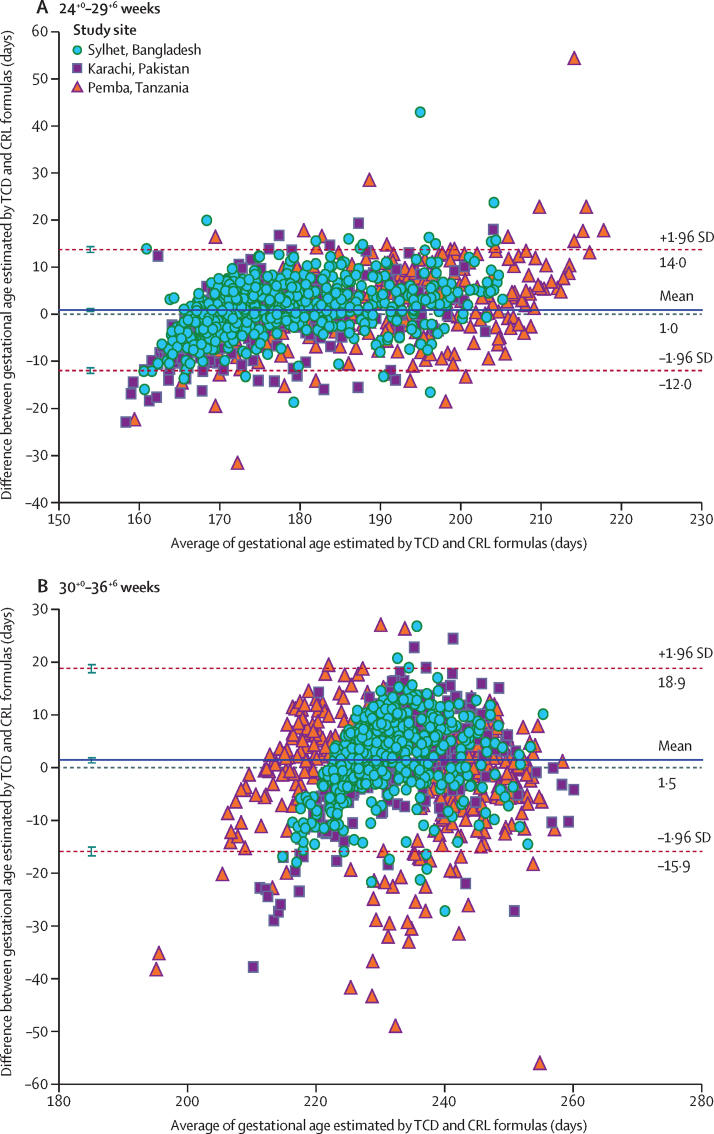
This prospective, population-based, cohort study was done in three LMICs (Bangladesh, Pakistan, and Tanzania) participating in the WHO Alliance for Maternal and Newborn Health Improvement study. Women carrying a live singleton fetus dated by crown-rump length (CRL) measurements between 8-14 weeks of gestation, who were willing to return for two additional ultrasound scans, and who planned on delivering in the study area were enrolled in the study. Participants underwent ultrasonography at 24-29 weeks and at 30-36 weeks' gestation. Birthweights were measured within 72 h of birth, and the proportions of infants who had a small-for-gestational-age birthweight (ie, a birthweight <10% of the standard birthweight for the infant's gestational age and sex according to the INTERGROWTH-21st project newborn baby reference standards) and appropriate-for-gestational-age birthweights were ascertained. Estimation of gestational age by standard fetal biometry measurements in addition to transcerebellar diameter (TCD) measurements was compared with gold-standard CRL measurements by use of Bland-Altman plots to calculate the mean difference and 95% limits of agreement. Statistical modelling was done to develop new gestational age prediction formulas for third trimester ultrasonography in LMICs.
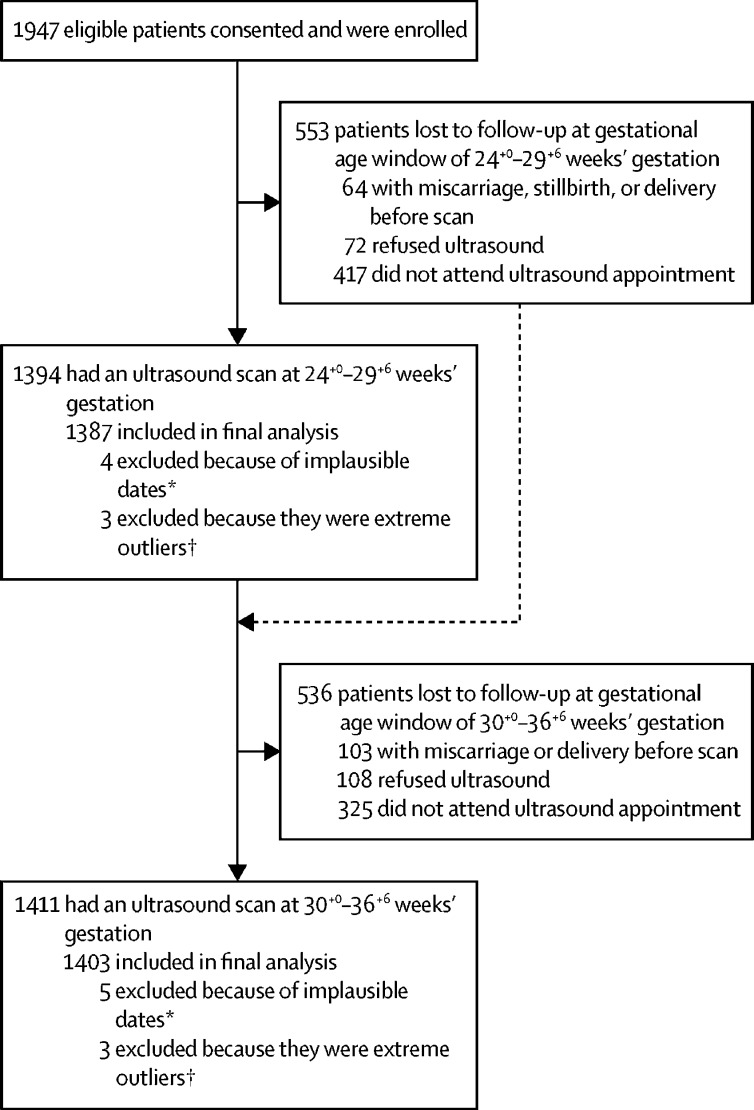
Between Feb 7, 2015, and Jan 9, 2017, 1947 women were enrolled in the study. 1387 pregnant women had an ultrasound scan at 24-29 weeks of gestation and 1403 had an ultrasound scan between 30-36 weeks of gestation. Of the 1379 unique infants whose birthweights were available, 981 (71·1%) infants were born with an appropriate-for-gestational-age birthweight and 398 (28·9%) infants were born with a small-for-gestational-age birthweight. The accuracy of late pregnancy ultrasound biometry using existing formulas to estimate gestational age in LMICs was similar to that in high-income settings. With standard dating formulas, late pregnancy ultrasound at 24-29 weeks' gestation was accurate to within approximately plus or minus 2 weeks of the gold-standard CRL measurement of gestational age, and late pregnancy ultrasound was accurate to within ±3 weeks of the CRL measurement at 30-36 weeks' gestation. In infants who were ultimately born small for gestational age, individual parameters systematically underestimated gestational age, apart from TCD, which showed minimal bias. By use of a novel parsimonious model formula that combined TCD with femur length, gestational age at the 24 -29-week ultrasound scan was estimated to within ±10·5 days of the CRL measurement and estimated to within ±15·1 days of the CRL measurement at the 30-36-week ultrasound scan. Similar results were observed in infants who were small-for-gestational-age.
Incorporation of TCD and the use of new formulas in late pregnancy ultrasound scans could improve the accuracy of gestational age estimation in both appropriate-for-gestational-age and small-for-gestational-age infants in LMICs. Given the high rates of small-for-gestational-age infants in LMICs, these results might be especially relevant. Validation of this new formula in other LMIC populations is needed to establish whether the accuracy of the late pregnancy ultrasound can be narrowed to within approximately 2 weeks.
Bill & Melinda Gates Foundation.
我们旨在评估和提高在中低收入国家(LMIC)中妊娠晚期(即 24 周后)超声扫描估计胎龄的准确性,因为这些国家在妊娠前半期获得超声检查的机会很少,且宫内生长受限很普遍。
这是一项在三个参与世界卫生组织母婴健康改善联盟研究的 LMIC(孟加拉国、巴基斯坦和坦桑尼亚)中进行的前瞻性、基于人群的队列研究。研究对象为妊娠 8-14 周,通过头臀长(CRL)测量确定单胎活产,愿意进行两次额外的超声检查,并计划在研究区域分娩的孕妇。参与者在 24-29 周和 30-36 周进行超声检查。在出生后 72 小时内测量出生体重,并确定小胎龄出生体重(即出生体重<根据 INTERGROWTH-21st 项目新生儿参考标准,婴儿胎龄和性别的标准出生体重的 10%)和适当胎龄出生体重的婴儿比例。使用 Bland-Altman 图比较标准胎儿生物测量测量值加小脑横径(TCD)测量值与金标准 CRL 测量值,以计算平均差异和 95%的一致性界限。使用统计模型为 LMIC 的妊娠晚期超声检查开发新的胎龄预测公式。
在 2015 年 2 月 7 日至 2017 年 1 月 9 日期间,共纳入 1947 名妇女。1387 名孕妇在 24-29 周时进行了超声检查,1403 名孕妇在 30-36 周时进行了超声检查。在 1379 名有独特出生体重的婴儿中,981 名(71.1%)婴儿出生时体重适宜,398 名(28.9%)婴儿出生时体重过小。在 LMIC 中,使用现有公式进行妊娠晚期超声生物测量来估计胎龄的准确性与高收入环境相似。使用标准的日期公式,妊娠 24-29 周的妊娠晚期超声检查在金标准 CRL 测量的胎龄上下约 2 周内准确,妊娠 30-36 周的 CRL 测量上下约 3 周内准确。在最终出生体重较小的婴儿中,除 TCD 外,个别参数系统地低估了胎龄,而 TCD 显示出最小的偏差。使用一种新的简洁模型公式,将 TCD 与股骨长度相结合,在妊娠 24-29 周的超声检查中,胎龄估计值与 CRL 测量值相差±10.5 天,在妊娠 30-36 周的超声检查中,胎龄估计值与 CRL 测量值相差±15.1 天。在体重过小的婴儿中也观察到了类似的结果。
在妊娠晚期超声检查中加入 TCD 并使用新公式可以提高在 LMIC 中对适宜胎龄和体重过小的婴儿的胎龄估计的准确性。鉴于 LMIC 中小胎龄婴儿的高比例,这些结果可能尤其相关。需要在其他 LMIC 人群中验证这个新公式,以确定妊娠晚期超声的准确性是否可以缩小到大约 2 周。
比尔和梅琳达·盖茨基金会。