CEPED, Institut de Recherche Pour le Développement, Paris, France.
Institute of Child Health, University College London, London, UK.
BMJ Glob Health. 2020 Mar 3;5(3):e001915. doi: 10.1136/bmjgh-2019-001915. eCollection 2020.
Increases in facility deliveries in sub-Saharan Africa have not yielded expected declines in maternal mortality, raising concerns about the quality of care provided in facilities. The readiness of facilities at different health system levels to provide both emergency obstetric and newborn care (EmONC) as well as referral is unknown. We describe this combined readiness by facility level and region in Senegal.
For this cross-sectional study, we used data from nine Demographic and Health Surveys between 1992 and 2017 in Senegal to describe trends in location of births over time. We used data from the 2017 Service Provision Assessment to describe EmONC and emergency referral readiness across facility levels in the public system, where 94% of facility births occur. A national global positioning system facility census was used to map access from lower-level facilities to the nearest facility performing caesareans.
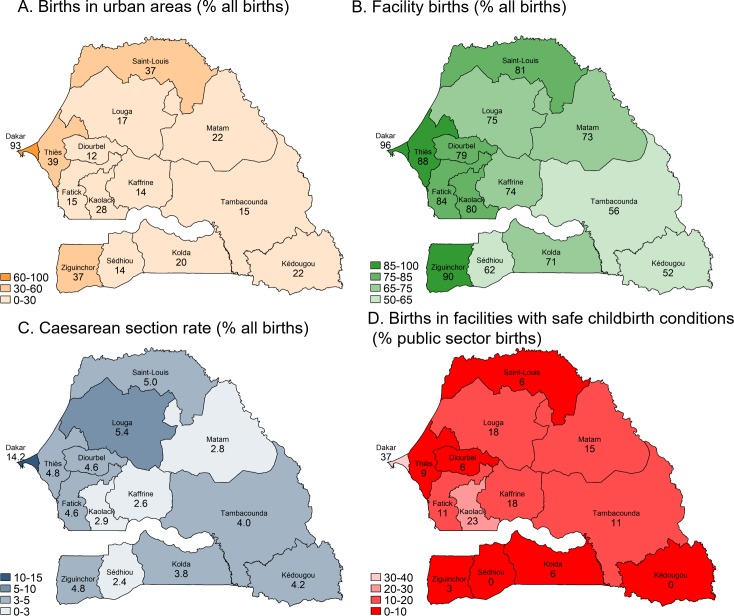
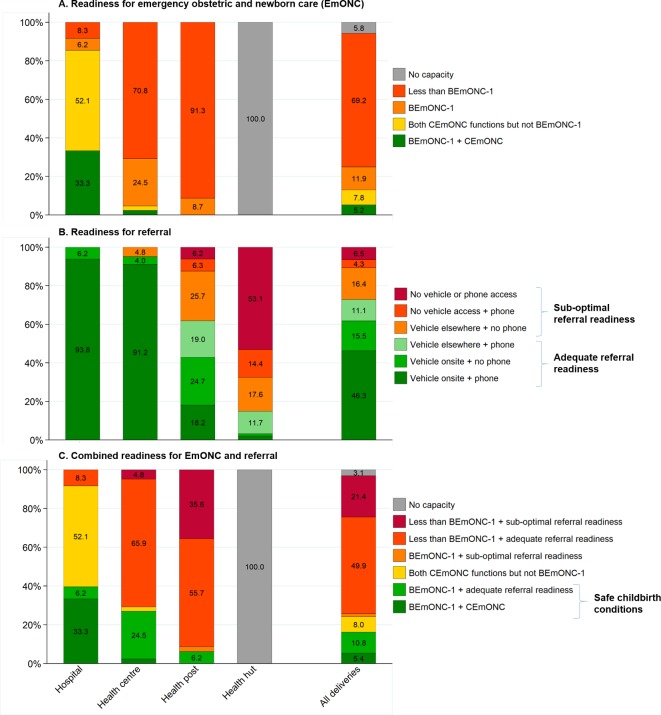
Births in facilities increased from 47% in 1992 to 80% in 2016, driven by births in lower-level health posts, where half of facility births now occur. Caesarean rates in rural areas more than doubled but only to 3.7%, indicating minor improvements in EmONC access. Only 9% of health posts had full readiness for basic EmONC, and 62% had adequate referral readiness (vehicle on-site or telephone and vehicle access elsewhere). Although public facilities accounted for three-quarters of all births in 2016, only 16% of such births occurred in facilities able to provide adequate combined readiness for EmONC and referral.
Our findings imply that many lower-level public facilities-the most common place of birth in Senegal-are unable to treat or refer women with obstetric complications, especially in rural areas. In light of rising lower-level facility births in Senegal and elsewhere, improvements in EmONC and referral readiness are urgently needed to accelerate reductions in maternal and perinatal mortality.
撒哈拉以南非洲地区医疗机构分娩量的增加并未如预期般降低产妇死亡率,这引发了人们对医疗机构提供的护理质量的担忧。不同卫生系统级别的医疗机构在提供紧急产科和新生儿护理(EmONC)以及转介服务方面的准备情况尚不清楚。我们在塞内加尔按医疗机构级别和地区对这种综合准备情况进行了描述。
在这项横断面研究中,我们使用了塞内加尔 1992 年至 2017 年期间的 9 次人口与健康调查的数据,以描述随时间推移的分娩地点趋势。我们使用 2017 年服务提供情况评估的数据,描述了公立系统中各级医疗机构提供 EmONC 和紧急转介服务的准备情况,因为 94%的医疗机构分娩都发生在公立系统中。利用国家全球定位系统设施普查数据,绘制了从较低级别设施到最近能进行剖腹产的设施的可达性地图。
1992 年至 2016 年期间,医疗机构分娩量从 47%增至 80%,这主要得益于基层卫生所分娩量的增加,现在有一半的医疗机构分娩都发生在基层卫生所。农村地区的剖腹产率增加了一倍多,但仅增加到 3.7%,表明 EmONC 服务的可及性略有改善。只有 9%的卫生所具备基本 EmONC 的全面准备,62%的卫生所具备适当的转介准备(现场有车辆或电话,其他地方有车辆)。尽管 2016 年公立医疗机构占所有分娩的四分之三,但只有 16%的分娩发生在能够提供充分的 EmONC 和转介综合准备的医疗机构中。
我们的研究结果表明,塞内加尔大多数常见的分娩地点——许多基层公立医疗机构——无法治疗或转介患有产科并发症的妇女,尤其是在农村地区。鉴于塞内加尔和其他地方基层医疗机构分娩量的增加,迫切需要提高 EmONC 和转介服务的准备情况,以加速降低产妇和围产期死亡率。