Department of Gastroenterology and Hepatology, Kindai University Faculty of Medicine, Osaka-Sayama 589-8511, Japan.
Clinical Research Center, Kindai University Hospital, Osaka-Sayama 589-8511, Japan.
World J Gastroenterol. 2020 Mar 7;26(9):947-959. doi: 10.3748/wjg.v26.i9.947.
Although several techniques for endoscopic ultrasound-guided biliary drainage (EUS-BD) are available at present, an optimal treatment algorithm of EUS-BD has not yet been established.
To evaluate the clinical utility of treatment method conversion during single endoscopic sessions for difficult cases in initially planned EUS-BD.
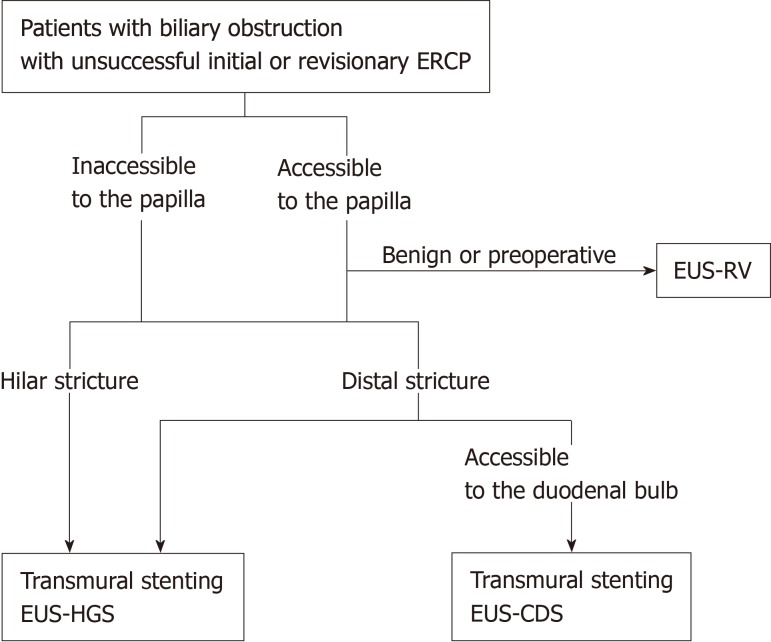
This was a single-center retrospective analysis using a prospectively accumulated database. Patients with biliary obstruction undergoing EUS-BD between May 2008 and April 2016 were included. The primary outcome was to evaluate the improvement in EUS-BD success rates by converting the treatment methods during a single endoscopic session. Secondary outcomes were clarification of the factors leading to the conversion from the initial EUS-BD and the assessment of efficacy and safety of the conversion as judged by technical success, clinical success, and adverse events (AEs).
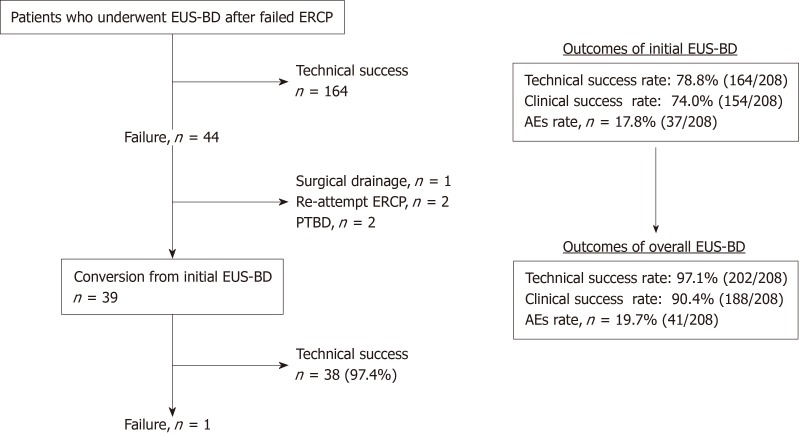
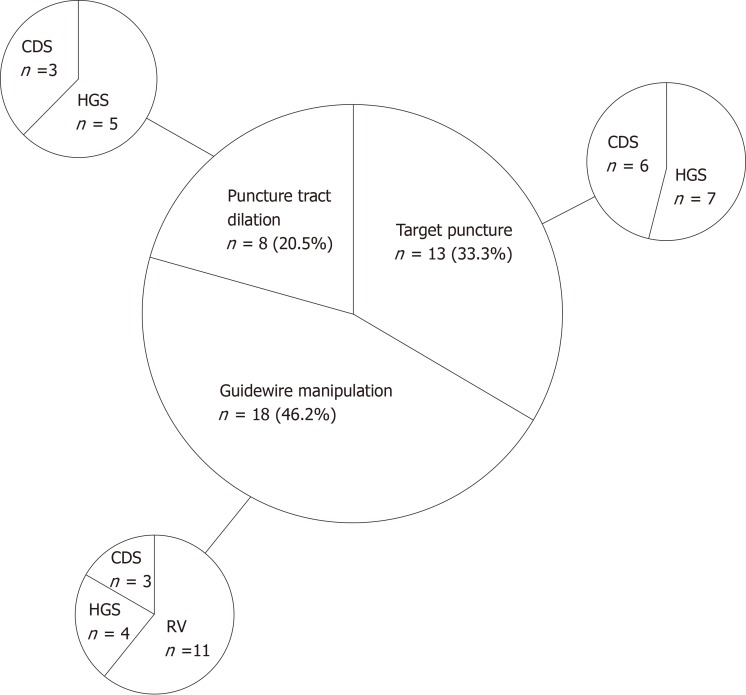
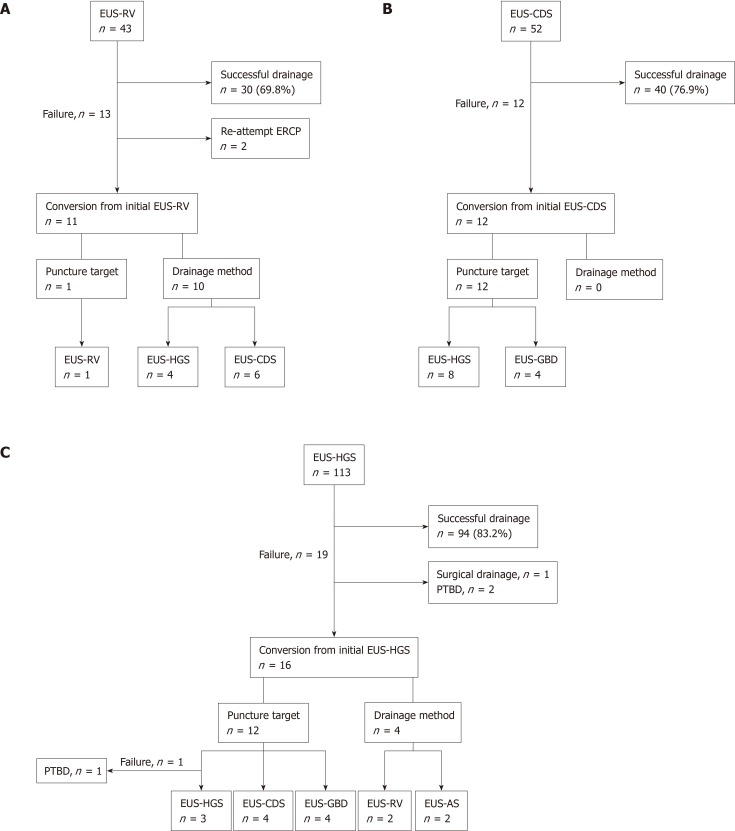
A total of 208 patients underwent EUS-BD during the study period. For 18.8% (39/208) of the patients, the treatment methods were converted to another EUS-BD technique from the initial plan. Biliary obstruction was caused by pancreatobiliary malignancies, other malignant lesions, biliary stones, and other benign lesions in 22, 11, 4, and 2 patients, respectively. The reasons for the difficulty with the initial EUS-BD were classified into the following 3 procedures: Target puncture ( = 13), guidewire manipulation ( = 18), and puncture tract dilation ( = 8). Technical success was achieved in 97.4% (38/39) of the cases and clinical success was achieved in 89.5% of patients (34/38). AEs occurred in 10.3% of patients, including bile leakage ( = 2), bleeding ( = 1), and cholecystitis ( = 1). The puncture target and drainage technique were altered in subsequent EUS-BD procedures in 25 and 14 patients, respectively. The final technical success rate with 95%CI for all 208 cases was 97.1% (95%CI: 93.8%-98.9%), while that of the initially planned EUS-BD was 78.8% (95%CI: 72.6%-84.2%).
Among multi-step procedures in EUS-BD, guidewire manipulation appeared to be the most technically challenging. When initially planned EUS-BD is technically difficult, treatment method conversion in a single endoscopic session may result in successful EUS-BD without leading to severe AEs.
目前有几种内镜超声引导下胆道引流(EUS-BD)技术,但尚未建立 EUS-BD 的最佳治疗方案。
评估在最初计划的 EUS-BD 中,对于困难病例,在单次内镜检查中转换治疗方法的临床实用性。
这是一项使用前瞻性累积数据库的单中心回顾性分析。纳入 2008 年 5 月至 2016 年 4 月期间因胆道梗阻而行 EUS-BD 的患者。主要结局是通过在单次内镜检查中转换治疗方法,评估 EUS-BD 成功率的提高。次要结局是明确从初始 EUS-BD 转换的原因,以及根据技术成功率、临床成功率和不良事件(AE)评估转换的疗效和安全性。
研究期间共有 208 例患者接受 EUS-BD。18.8%(39/208)的患者从初始计划中转用另一种 EUS-BD 技术。引起胆道梗阻的原因分别为胰胆管恶性肿瘤、其他恶性病变、胆管结石和其他良性病变的患者分别为 22、11、4 和 2 例。初始 EUS-BD 困难的原因分为以下 3 个步骤:靶位穿刺(=13)、导丝操作(=18)和穿刺道扩张(=8)。38 例(97.4%)患者技术成功,34 例(89.5%)患者临床成功。10.3%的患者出现 AE,包括胆漏(=2)、出血(=1)和胆囊炎(=1)。25 例患者在后续 EUS-BD 中改变了穿刺靶点,14 例患者改变了引流技术。所有 208 例患者的最终技术成功率为 97.1%(95%CI:93.8%-98.9%),而初始计划 EUS-BD 的技术成功率为 78.8%(95%CI:72.6%-84.2%)。
在 EUS-BD 的多步骤操作中,导丝操作似乎是最具技术挑战性的。当最初计划的 EUS-BD 技术上困难时,在单次内镜检查中转换治疗方法可能会导致 EUS-BD 成功,而不会导致严重的 AE。