Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, Hospital of the University of Pennsylvania, 839 W. Gates, 3600 Spruce Street, Philadelphia, PA, 19103-4283, USA.
Palliative and Advanced Illness Research (PAIR) Center, University of Pennsylvania, Philadelphia, PA, USA.
Intensive Care Med. 2020 Jun;46(6):1222-1231. doi: 10.1007/s00134-020-06010-9. Epub 2020 Mar 23.
Previous studies assessing impact of acute respiratory distress syndrome (ARDS) on mortality have shown conflicting results. We sought to assess the independent association of ARDS with in-hospital mortality among intensive care unit (ICU) patients with sepsis.
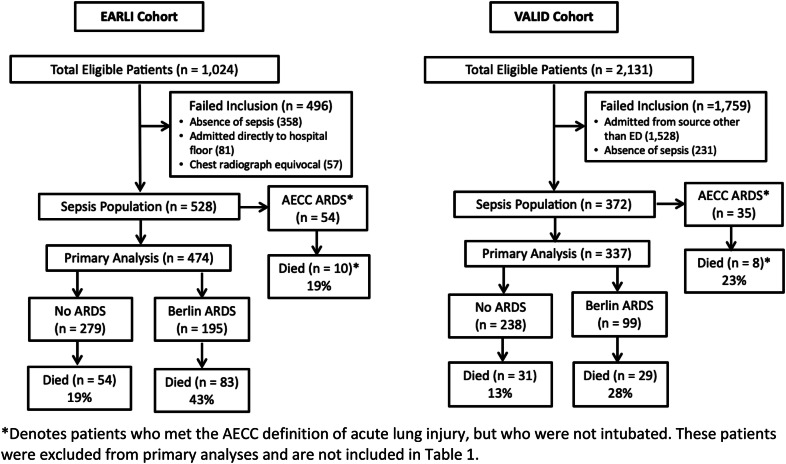
We studied two prospective sepsis cohorts drawn from the Early Assessment of Renal and Lung Injury (EARLI; n = 474) and Validating Acute Lung Injury markers for Diagnosis (VALID; n = 337) cohorts. ARDS was defined by Berlin criteria. We used logistic regression to compare in-hospital mortality in patients with and without ARDS, controlling for baseline severity of illness. We also estimated attributable mortality, adjusted for illness severity by stratification.
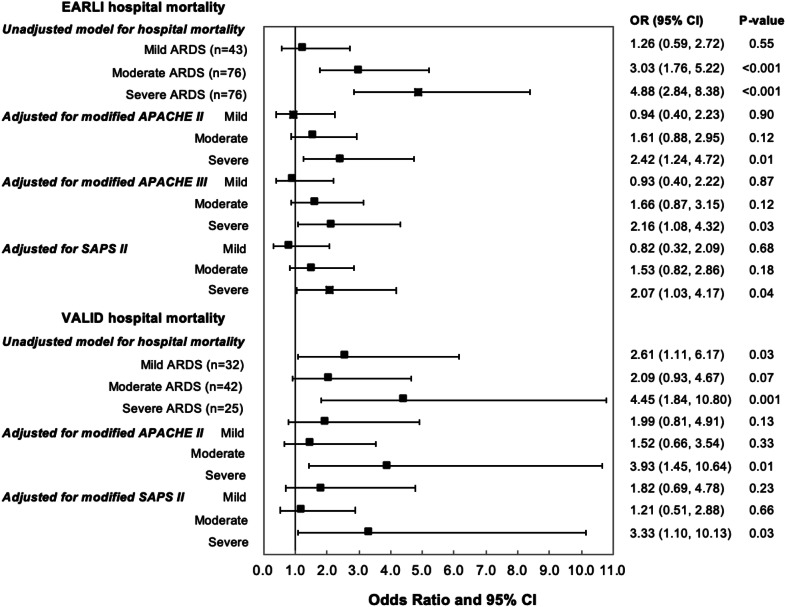
ARDS occurred in 195 EARLI patients (41%) and 99 VALID patients (29%). ARDS was independently associated with risk of hospital death in multivariate analysis, even after controlling for severity of illness, as measured by APACHE II (odds ratio [OR] 1.65 (95% confidence interval [CI] 1.02, 2.67), p = 0.04 in EARLI; OR 2.12 (CI 1.16, 3.92), p = 0.02 in VALID). Patients with severe ARDS (P/F < 100) primarily drove this relationship. The attributable mortality of ARDS was 27% (CI 14%, 37%) in EARLI and 37% (CI 10%, 51%) in VALID. ARDS was independently associated with ICU mortality, hospital length of stay (LOS), ICU LOS, and ventilator-free days.
Development of ARDS among ICU patients with sepsis confers increased risk of ICU and in-hospital mortality in addition to other important outcomes. Clinical trials targeting patients with severe ARDS will be best poised to detect measurable differences in these outcomes.
先前评估急性呼吸窘迫综合征(ARDS)对死亡率影响的研究结果存在矛盾。我们旨在评估 ARDS 与脓毒症重症监护病房(ICU)患者院内死亡率的独立相关性。
我们研究了两个前瞻性脓毒症队列,分别来自早期肾和肺损伤评估(EARLI;n=474)和急性肺损伤标志物验证用于诊断(VALID;n=337)队列。ARDS 按照柏林标准定义。我们使用逻辑回归比较 ARDS 患者和非 ARDS 患者的院内死亡率,同时控制基线疾病严重程度。我们还通过分层调整疾病严重程度来估计归因死亡率。
EARLI 中有 195 名(41%)和 VALID 中有 99 名(29%)患者发生 ARDS。即使在控制 APACHE II 评分(EARLI 中的比值比 [OR] 1.65(95%置信区间 [CI] 1.02,2.67),p=0.04;VALID 中的 OR 2.12(CI 1.16,3.92),p=0.02)评估的疾病严重程度后,ARDS 在多变量分析中仍与住院死亡风险独立相关。患有严重 ARDS(P/F<100)的患者主要导致了这种关系。EARLI 中的 ARDS 归因死亡率为 27%(CI 14%,37%),VALID 中的 ARDS 归因死亡率为 37%(CI 10%,51%)。ARDS 与 ICU 死亡率、住院时间(LOS)、ICU LOS 和无呼吸机天数独立相关。
在脓毒症 ICU 患者中发生 ARDS 除了其他重要结局外,还会增加 ICU 和院内死亡率的风险。针对严重 ARDS 患者的临床试验将最有能力检测这些结局的可衡量差异。