Department of Social Medicine and Health Service Management, Army Medical University (Third Military Medical University), No.30 Gaotanyan Road, Shapingba District, Chongqing, 400038, China.
Tuwai community health service center, Shapingba District, Chongqing, China.
BMC Health Serv Res. 2020 Mar 24;20(1):247. doi: 10.1186/s12913-020-05120-w.
Equalizing basic public health services (BPHS) for all has been one goal of the health system reform in China since 2009. At the end of the 12th five-year plan, we conducted a series of surveys to understand BPHS implementation in Southwest China, and firstly reported implementation of health education (HE) and explore the barriers to HE delivery.
Mixed research methods were used to investigate achievement in and barriers to HE in Southwest China. SPSS 22.0 was used for data analysis.
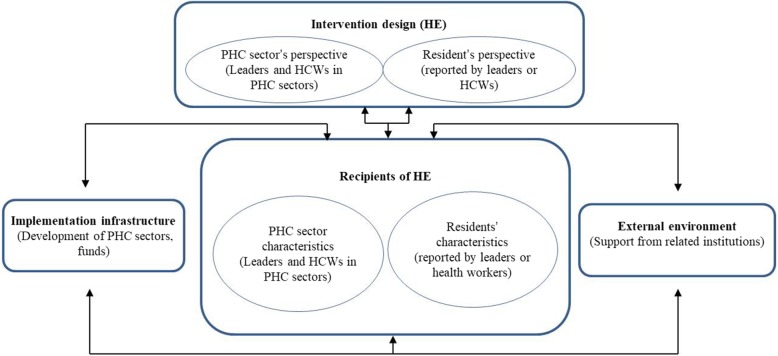
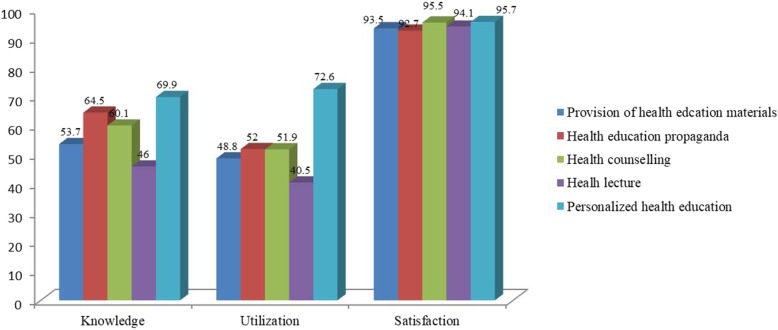
Nine hundred and eighty-nine residents were surveyed by questionnaire. 16 health care workers (HCWs) and 16 directors from 16 PHC sectors were included in the in-depth interviews. Less than 50% of residents who knew or utilized some item of HE. Age, residence, region (Chongqing or Guizhou), marital status, education, occupation, type and quality of primary health care (PHC) sectors to deliver BPHS, self-reported health and status of chronic diseases were associated with knowledge or utilization of HE. Distance to PHC sectors was associated with the knowledge of HE, gender and health insurance were associated with utilization of HE. Age, marital status, occupation region and self-reported health were associated with satisfaction regarding HE. Barriers to HE delivery included defects in HE design, weak capacity in PHC sectors to provide HE, residents' poor cooperation, lack of multi-sector cooperation, poor equipment and weak health system.
Southwest China delivered HE in all PHC sectors. However, our study underlined many barriers to equalization of HE. To address those barriers and achieve HE quality improvement, comprehensive measures to improve capacity of PHC sectors, enhance multi-sector cooperation and strengthen health information systems are all urgent needs.
自 2009 年以来,实现基本公共卫生服务均等化一直是中国卫生体制改革的目标之一。在十二五规划末期,我们进行了一系列调查,以了解中国西南地区基本公共卫生服务的实施情况,并首次报告了健康教育的实施情况,并探讨了其实施障碍。
采用混合研究方法调查中国西南地区健康教育的实施情况和障碍。采用 SPSS 22.0 进行数据分析。
共调查了 989 名居民,对 16 名卫生保健工作者(HCWs)和 16 名来自 16 个基层医疗部门的主任进行了深入访谈。不到 50%的居民了解或使用过某些健康教育项目。年龄、居住地、地区(重庆或贵州)、婚姻状况、教育程度、职业、提供基本公共卫生服务的基层医疗部门的类型和质量、自我报告的健康状况和慢性病状况与对健康教育的知识或利用有关。到基层医疗部门的距离与对健康教育的了解有关,性别和医疗保险与对健康教育的利用有关。年龄、婚姻状况、职业地区和自我报告的健康状况与对健康教育的满意度有关。健康教育实施的障碍包括健康教育设计缺陷、基层医疗部门提供健康教育的能力薄弱、居民合作不佳、多部门合作缺乏、设备差和卫生系统薄弱。
中国西南地区在所有基层医疗部门都开展了健康教育。然而,我们的研究强调了健康教育均等化的许多障碍。为了解决这些障碍,提高健康教育质量,全面提高基层医疗部门的能力,加强多部门合作,加强卫生信息系统建设都是迫切需要的。