Department of Anatomy and Neurosciences, Amsterdam Neuroscience, Amsterdam UMC, Vrije Universiteit Amsterdam, P.O. Box 7057, 1007, MB, Amsterdam, the Netherlands.
Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam, the Netherlands.
Acta Neuropathol Commun. 2020 Mar 26;8(1):39. doi: 10.1186/s40478-020-00914-9.
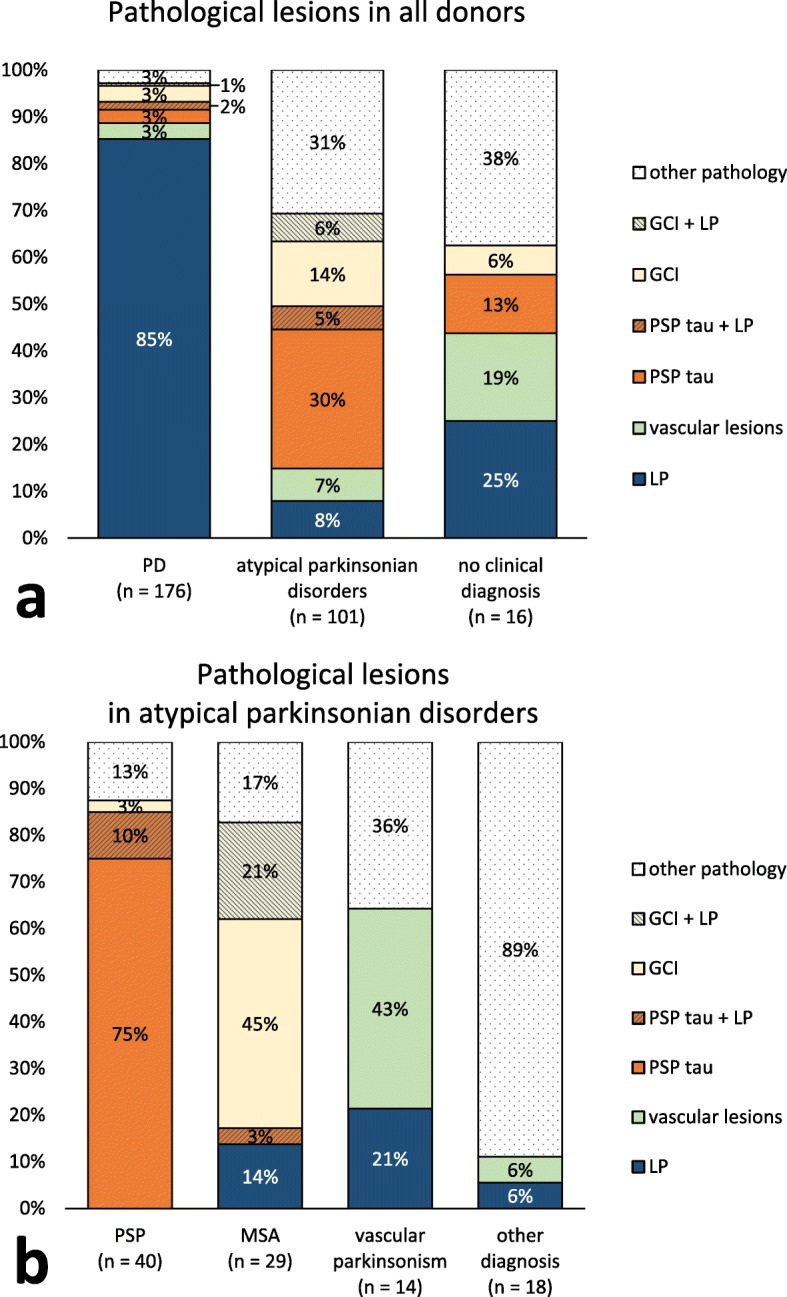
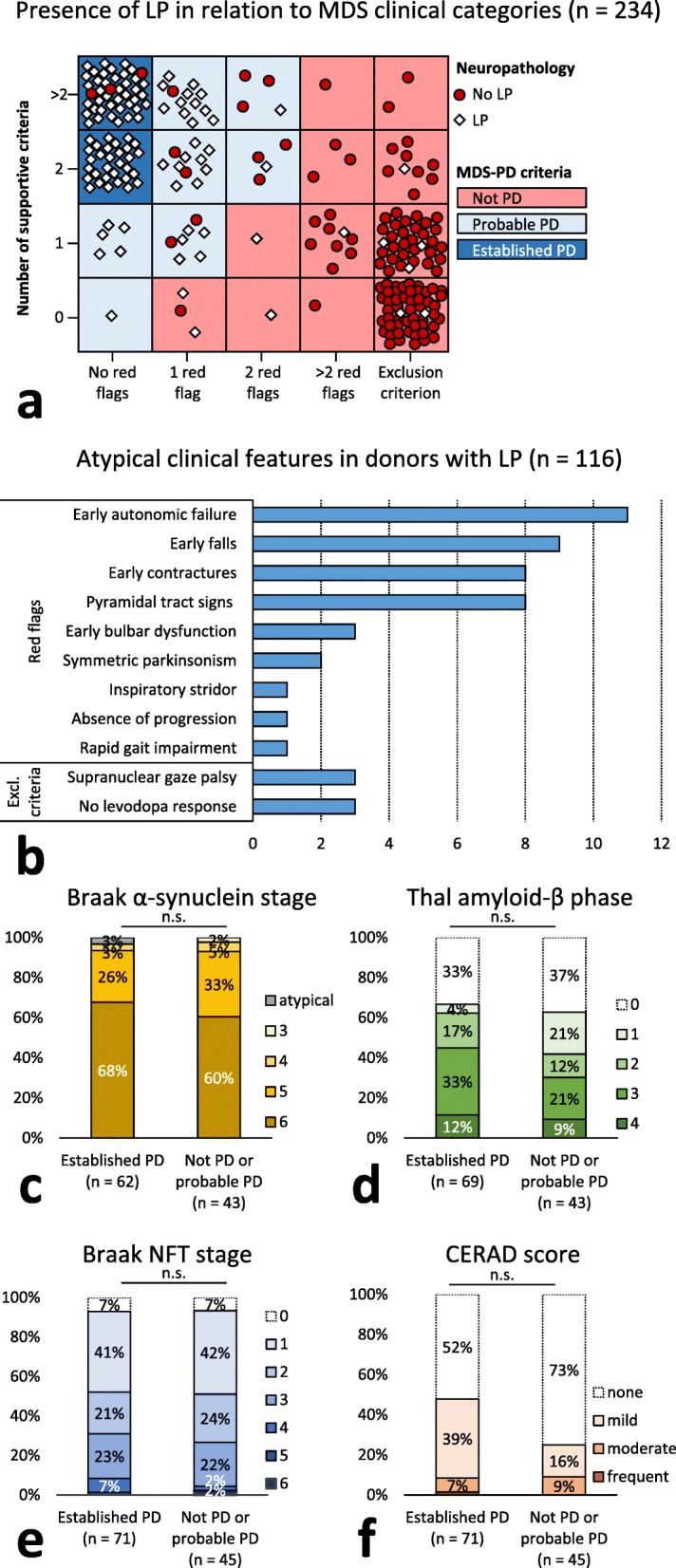
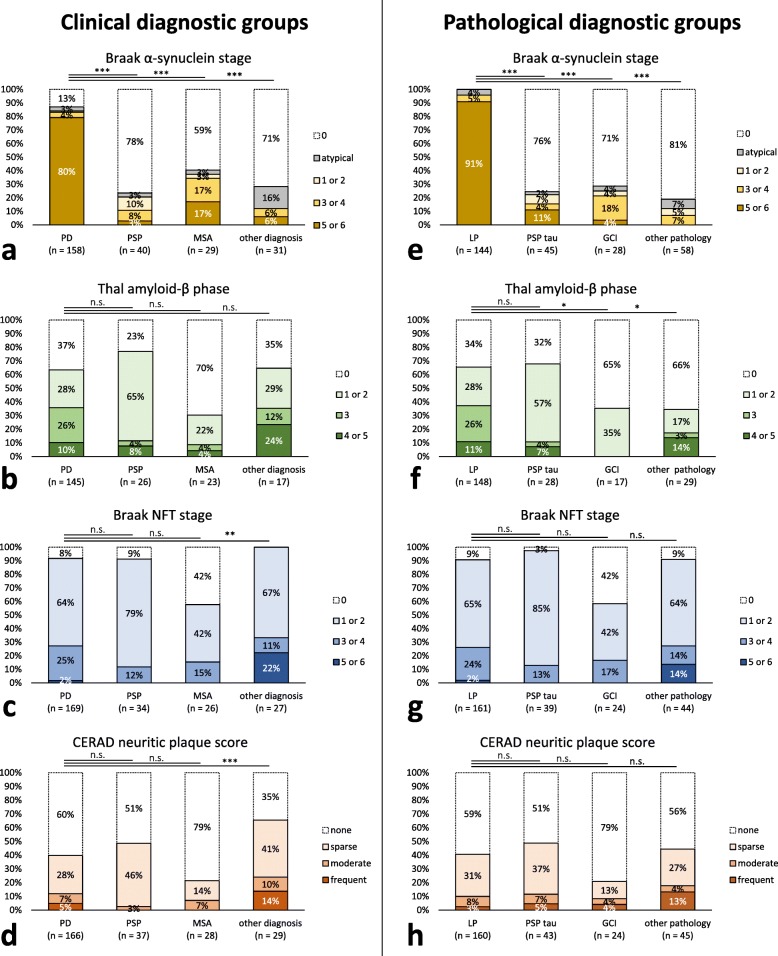
The clinical diagnosis in patients with parkinsonian disorders can be challenging, and a definite diagnosis requires neuropathological confirmation. The aim of this study was to examine whether a clinical diagnosis of Parkinson's disease (PD) and atypical parkinsonian disorders predict the presence of Lewy pathology (LP) and concomitant neuropathological lesions.We included 293 donors with a history of parkinsonism without dementia at disease onset, collected by the Netherlands Brain Bank (NBB) from 1989 to 2015. We retrospectively categorized donors according the International Parkinson and Movement Disorder Society clinical diagnostic criteria for PD (MDS-PD criteria) as 'not PD', 'probable PD' or 'established PD'. We compared the final clinical diagnosis to presence of neuropathological lesions as defined by BrainNet Europe and National Institute on Aging - Alzheimer's Association guidelines.LP was present in 150 out of 176 donors (85%) with a clinical diagnosis of PD, in 8 out of 101 donors (8%) with atypical parkinsonian disorders and in 4 out of 16 donors (25%) without a definite clinical diagnosis. Independent from age at death, stages of amyloid-β, but not neurofibrillary tau or neuritic plaques, were higher in donors with LP compared to other types of pathology (p = 0.009). The MDS-PD criteria at a certainty level of 'probable PD' predicted presence of LP with a diagnostic accuracy of 89.3%. Among donors with LP, 'established PD' donors showed similar Braak α-synuclein stages and stages of amyloid-β, neurofibrillary tau and neuritic plaques compared to 'not PD' or 'probable PD' donors.In conclusion, both a clinical diagnosis of PD as well as MDS-PD criteria accurately predicted presence of LP in NBB donors. LP was associated with more widespread amyloid-β pathology, suggesting a link between amyloid-β accumulation and LP formation.
在帕金森病患者中,临床诊断可能具有挑战性,明确的诊断需要神经病理学证实。本研究旨在探讨帕金森病(PD)和非典型帕金森病的临床诊断是否能预测路易体病理(LP)和伴随的神经病理学病变的存在。我们纳入了 293 名在发病时无痴呆的帕金森病病史的供体,这些供体由荷兰脑库(NBB)于 1989 年至 2015 年收集。我们回顾性地根据国际帕金森病和运动障碍协会的 PD 临床诊断标准(MDS-PD 标准)将供体分为“非 PD”、“可能 PD”或“确诊 PD”。我们将最终的临床诊断与欧洲脑网络和美国国立老化研究所-阿尔茨海默病协会指南定义的神经病理学病变进行比较。在临床诊断为 PD 的 176 名供体中有 150 名(85%)存在 LP,在 101 名非典型帕金森病供体中有 8 名(8%)存在 LP,在 16 名无明确临床诊断的供体中有 4 名(25%)存在 LP。与其他类型的病理学相比,无论死亡时的年龄如何,LP 供体的淀粉样蛋白-β、但不是神经纤维缠结 tau 或神经原纤维缠结斑块的分期更高(p=0.009)。在确定性水平为“可能 PD”的 MDS-PD 标准预测 LP 的存在,其诊断准确性为 89.3%。在存在 LP 的供体中,与“非 PD”或“可能 PD”供体相比,“确诊 PD”供体的 Braak α-突触核蛋白分期和淀粉样蛋白-β、神经纤维缠结 tau 和神经原纤维缠结斑块的分期相似。总之,在 NBB 供体中,PD 的临床诊断和 MDS-PD 标准均能准确预测 LP 的存在。LP 与更广泛的淀粉样蛋白-β病理学相关,提示淀粉样蛋白-β 积累与 LP 形成之间存在联系。