Murthy Rashmi K, Song Juhee, Raghavendra Akshara S, Li Yisheng, Hsu Limin, Hess Kenneth R, Barcenas Carlos H, Valero Vicente, Carlson Robert W, Tripathy Debu, Hortobagyi Gabriel N
1Department of Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX USA.
2Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX USA.
NPJ Breast Cancer. 2020 Mar 25;6:11. doi: 10.1038/s41523-020-0152-4. eCollection 2020.
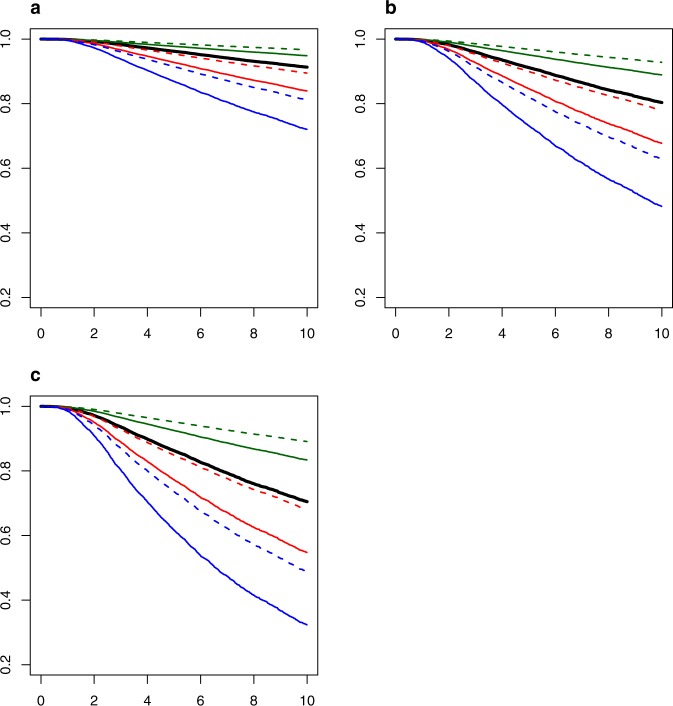
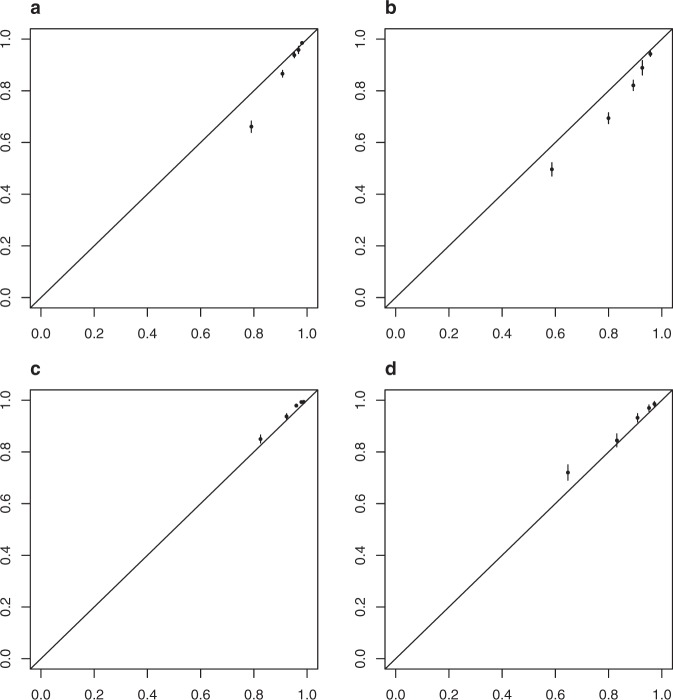
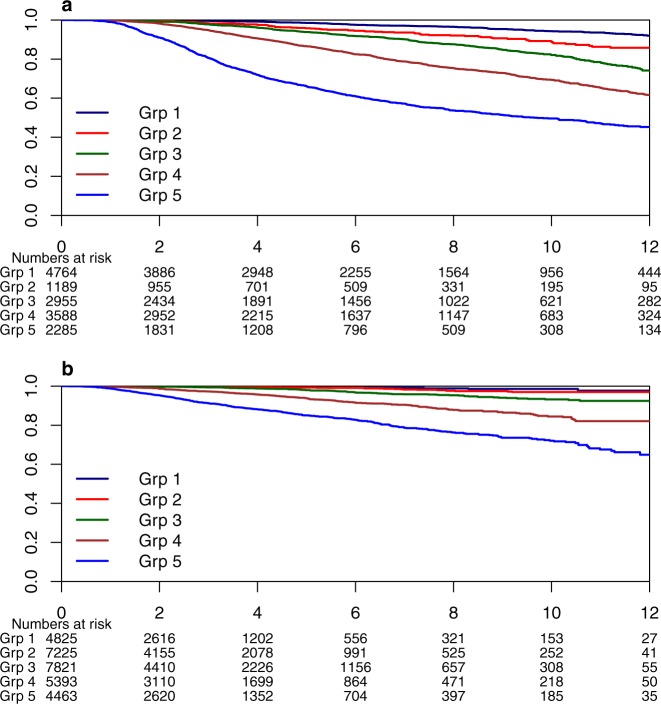
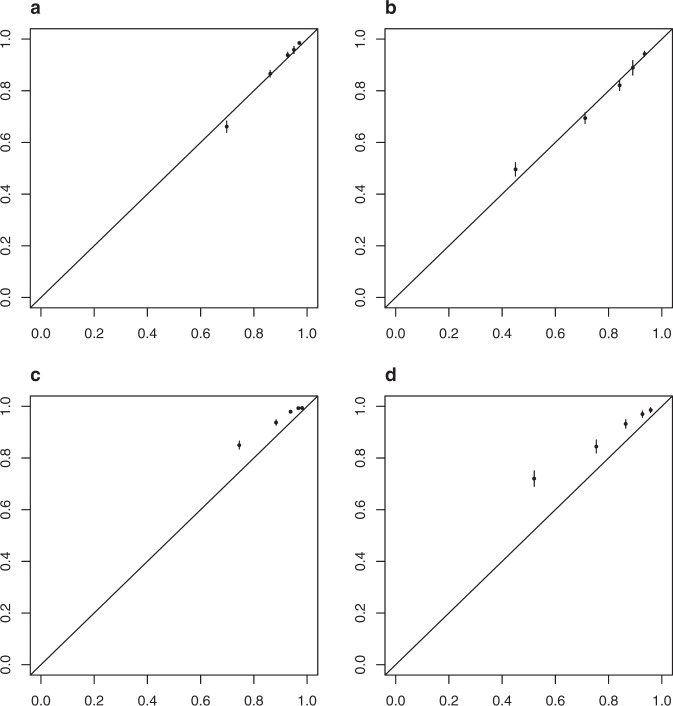
We developed prognostic models for breast cancer-specific survival (BCSS) that consider anatomic stage and other important determinants of prognosis and survival in breast cancer, such as age, grade, and receptor-based subtypes with the intention to demonstrate that these factors, conditional on stage, improve prediction of BCSS. A total of 20,928 patients with stage I-III invasive primary breast cancer treated at The University of Texas MD Anderson Cancer Center between 1990 and 2016, who received surgery as an initial treatment were identified to generate prognostic models by Fine-Gray competing risk regression model. Model predictive accuracy was assessed using Harrell's C-index. The Aalen-Johansen estimator and a selected Fine-Gray model were used to estimate the 5-year and 10-year BCSS probabilities. The performance of the selected model was evaluated by assessing discrimination and prediction calibration in an external validation dataset of 29,727 patients from the National Comprehensive Cancer Network (NCCN). The inclusion of age, grade, and receptor-based subtype in addition to stage significantly improved the model predictive accuracy (C-index: 0.774 (95% CI 0.755-0.794) vs. 0.692 for stage alone, < 0.0001). Young age (<40), higher grade, and TNBC subtype were significantly associated with worse BCSS. The selected model showed good discriminative ability but poor calibration when applied to the validation data. After recalibration, the predictions showed good calibration in the training and validation data. More refined BCSS prediction is possible through a model that has been externally validated and includes clinical and biological factors.
我们开发了乳腺癌特异性生存(BCSS)的预后模型,该模型考虑了解剖学分期以及乳腺癌预后和生存的其他重要决定因素,如年龄、分级和基于受体的亚型,目的是证明这些因素在分期的条件下可改善BCSS的预测。我们确定了1990年至2016年间在德克萨斯大学MD安德森癌症中心接受治疗的20928例I-III期浸润性原发性乳腺癌患者,这些患者接受手术作为初始治疗,并通过Fine-Gray竞争风险回归模型生成预后模型。使用Harrell's C指数评估模型预测准确性。使用Aalen-Johansen估计器和选定的Fine-Gray模型来估计5年和10年BCSS概率。在来自国家综合癌症网络(NCCN)的29727例患者的外部验证数据集中,通过评估区分度和预测校准来评估选定模型的性能。除分期外,纳入年龄、分级和基于受体的亚型显著提高了模型预测准确性(C指数:0.774(95%CI 0.755-0.794),而仅分期为0.692,P<0.0001)。年轻(<40岁)、高分级和三阴性乳腺癌(TNBC)亚型与较差的BCSS显著相关。选定的模型在应用于验证数据时显示出良好的区分能力,但校准较差。重新校准后,预测在训练和验证数据中显示出良好的校准。通过经过外部验证并包括临床和生物学因素的模型,可以实现更精确的BCSS预测。