El Damaty Ahmed, Marx Sascha, Cohrs Gesa, Vollmer Marcus, Eltanahy Ahmed, El Refaee Ehab, Baldauf Joerg, Fleck Steffen, Baechli Heidi, Zohdi Ahmed, Synowitz Michael, Unterberg Andreas, Schroeder Henry W S
Department of Neurosurgery, Heidelberg University Hospital, Im Neuenheimer Feld 400, 69120, Heidelberg, Germany.
Department of Neurosurgery, University Medicine Greifswald, Greifswald, Germany.
Childs Nerv Syst. 2020 Nov;36(11):2725-2731. doi: 10.1007/s00381-020-04585-8. Epub 2020 Mar 28.
Age and etiology play a crucial role in success of endoscopic third ventriculostomy (ETV) as a treatment of obstructive hydrocephalus. Outcome is worse in infants, and controversies still exist whether ETV is superior to shunt placement. We retrospectively analyzed 70 patients below 2 years from 4 different centers treated with ETV and assessed success.
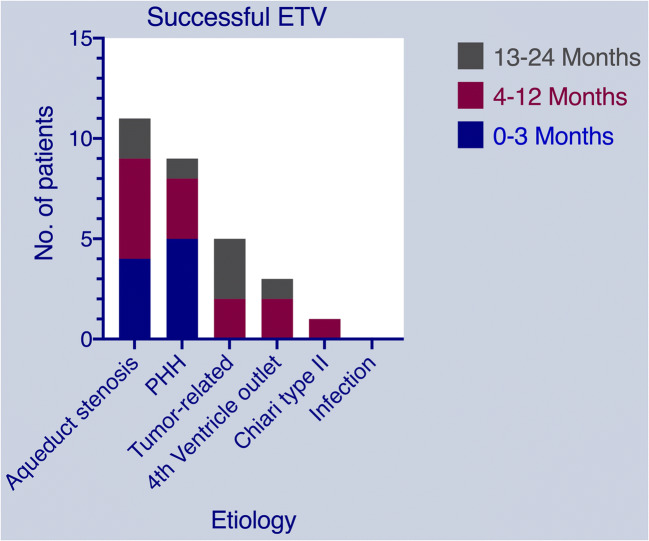
Children < 2 years who received an ETV within 1994-2018 were included. Patients were classified according to age and etiology; < 3, 4-12, and 13-24 months, etiologically; aqueductal stenosis, post-hemorrhagic-hydrocephalus (PHH), tumor-related, fourth ventricle outflow obstruction, with Chiari-type II and following CSF infection. We investigated statistically the predictors for ETV success through computing Kaplan-Meier estimates using patient's follow-up time and time to ETV failure.
We collected 70 patients. ETV success rate was 41.4%. The highest rate was in tumor-related hydrocephalus and fourth ventricle outlet obstruction (62.5%, 60%) and the lowest rate was in Chiari-type II and following infection (16.7%, 0%). The below 3 months age group showed relatively lower success rate (33.3%) in comparison to older groups which showed similar results (46.4%, 46.6%). Statistically, a previous VP shunt was a predictor for failure (p value < 0.05).
Factors suggesting a high possibility of failure were age < 3 months and etiology such as Chiari-type II or following infection. Altered CSF dynamics in patients with PHH and under-developed arachnoid villi may play a role in ETV failure. We do not recommend ETV as first line in children < 3 months of age or in case of Chiari II or following infection.
年龄和病因在内镜下第三脑室造瘘术(ETV)治疗梗阻性脑积水的成功率中起着关键作用。婴儿的治疗效果较差,ETV是否优于分流术仍存在争议。我们回顾性分析了来自4个不同中心接受ETV治疗的70例2岁以下患者,并评估了成功率。
纳入1994年至2018年期间接受ETV治疗的2岁以下儿童。患者根据年龄和病因进行分类;年龄方面分为<3个月、4 - 12个月和13 - 24个月,病因方面分为导水管狭窄、出血后脑积水(PHH)、肿瘤相关、第四脑室流出道梗阻、Chiari II型及继发脑脊液感染。我们通过使用患者的随访时间和ETV失败时间计算Kaplan - Meier估计值,对ETV成功的预测因素进行了统计学研究。
我们收集了70例患者。ETV成功率为41.4%。最高成功率出现在肿瘤相关脑积水和第四脑室出口梗阻(62.5%,60%),最低成功率出现在Chiari II型及继发感染(16.7%,0%)。与年龄较大的组(成功率分别为46.4%,46.6%)相比,3个月以下年龄组的成功率相对较低(33.3%)。统计学上,既往脑室腹腔分流术(VP分流术)是失败的一个预测因素(p值<0.05)。
提示失败可能性高的因素是年龄<3个月以及Chiari II型或继发感染等病因。PHH患者脑脊液动力学改变和蛛网膜绒毛发育不全可能在ETV失败中起作用。我们不建议在3个月以下儿童或Chiari II型或继发感染的情况下将ETV作为一线治疗方法。