Faculty of Medicine, Department of Geriatrics, University of Turku, Turku City Hospital, Kunnallissairaalantie 20, FI-20700, Turku, Finland.
City of Turku, Welfare Division, Turku, Finland.
BMC Geriatr. 2020 Mar 30;20(1):120. doi: 10.1186/s12877-020-01516-9.
Despite a non-specific nature of self-rated health (SRH), it seems to be a strong predictor of mortality. The aim of this study is to assess the association of SRH and objective health status (OH) with all-cause mortality in 70-year-old community-dwelling older people in Finland.
A prospective study with 5-, 10- and 27-year follow-ups. SRH (n = 1008) was assessed with a single question and OH (n = 962) by the Rockwood's Frailty Index (FI). To assess the association of SRH and OH with mortality, Cox regression model was used.
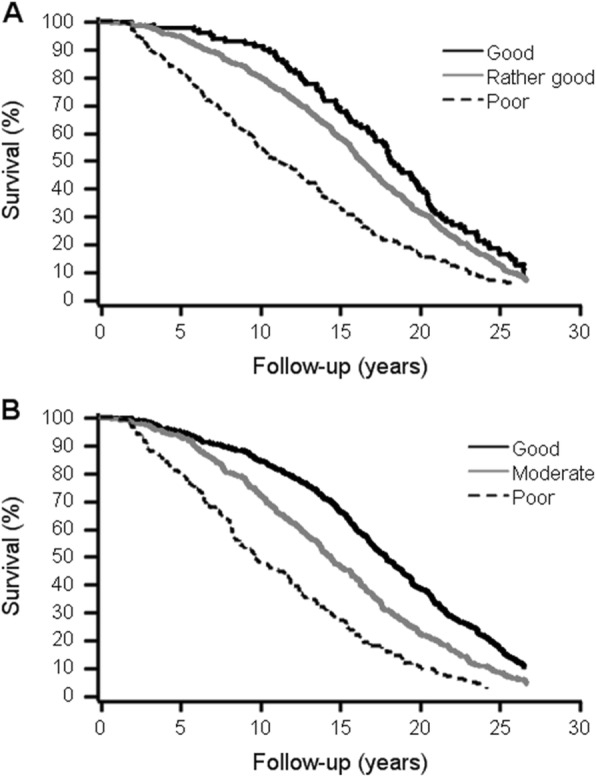
Of the 1008 participants, 138 (13.7%), 319 (31.6%), and 932 deceased (86.3%) during the 5-, 10- and 27-year follow-ups, respectively. In unadjusted models, subjects with poor SRH had almost eightfold risk for mortality compared to those with good SRH during the 5-year follow-up; among those with poor OH, the risk was fourfold compared to those with good OH. In the 10-year-follow up, both poor SRH and poor OH predicted about fourfold risk for mortality compared to those with good health. During the 27-year follow-up, OH was a stronger predictor of mortality than SRH. Poor SRH, compared to good SRH, showed 95% sensitivity and 34% specificity for 5-year mortality; corresponding figures for OH were 54 and 80%, respectively.
Single-item SRH seems to be able to capture almost the same as OH in predicting a short-term (less than 10 years) mortality risk among older adults in clinical settings. The use of SHR may also enhance the focus on patient-centered care.
尽管自我报告的健康状况(SRH)具有非特异性,但它似乎是死亡率的强有力预测指标。本研究旨在评估芬兰 70 岁社区居住的老年人的 SRH 和客观健康状况(OH)与全因死亡率之间的关系。
一项前瞻性研究,随访时间为 5 年、10 年和 27 年。使用单一问题评估 SRH(n=1008),使用 Rockwood 的虚弱指数(FI)评估 OH(n=962)。为了评估 SRH 和 OH 与死亡率的关系,使用 Cox 回归模型。
在 1008 名参与者中,分别有 138 名(13.7%)、319 名(31.6%)和 932 名(86.3%)在 5 年、10 年和 27 年随访期间死亡。在未调整的模型中,与良好 SRH 的参与者相比,SRH 较差的参与者在 5 年随访期间的死亡风险几乎高 8 倍;在 OH 较差的参与者中,与 OH 良好的参与者相比,死亡风险高 4 倍。在 10 年随访中,与健康状况良好的参与者相比,SRH 和 OH 均预测了约 4 倍的死亡风险。在 27 年随访期间,OH 是死亡率的更强预测指标,比 SRH 更为重要。与良好的 SRH 相比,不良的 SRH 在 5 年内预测死亡率的敏感性为 95%,特异性为 34%;OH 的相应数字分别为 54%和 80%。
单项 SRH 似乎能够在预测临床环境中老年人短期(<10 年)死亡风险方面,与 OH 一样有效。使用 SHR 还可以增强对以患者为中心的护理的关注。