Department of Clinical Pharmacy, OLVG, Amsterdam, The Netherlands.
Department of Surgery, OLVG, Amsterdam, The Netherlands.
PLoS One. 2020 Apr 2;15(4):e0229940. doi: 10.1371/journal.pone.0229940. eCollection 2020.
To identify the preventability, determinants and causes of unplanned hospital readmissions within 30 days of discharge using a multidisciplinary approach and including patients' perspectives.
A prospective cross-sectional single-center study.
Urban teaching hospital in Amsterdam, the Netherlands.
430 patients were included. Inclusion criteria were: age ≥ 18 years, discharged from one of seven participating clinical departments and an unplanned readmission within 30 days.
Residents from the participating departments individually assessed whether the readmission was caused by healthcare, the preventability and possible causes of readmissions using a tool. Thereafter, the preventability of the cases was discussed in a multidisciplinary meeting with residents of all participating departments and clinical pharmacists. The primary outcome was the proportion of readmissions that were potentially preventable. Secondary outcomes were the determinants for a readmission, causes for preventable readmissions, the change in the final decision on preventability after the multidisciplinary meeting and the value of patient interviews in assessing preventability. Differences in characteristics of potentially preventable readmissions (PPRs) and non-PPRs were analyzed using multivariable logistic regression.
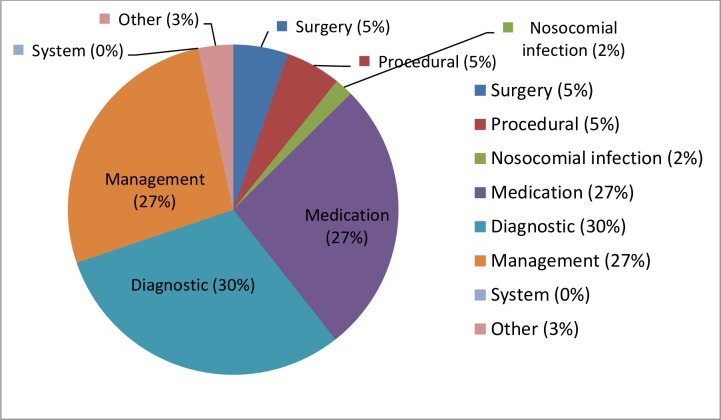
Of 430 readmissions, 56 (13%) were assessed as PPRs. Age was significantly associated with a PPR (adjusted OR: 2.42; 95%, CI 1.23-4.74; p = 0.01). The main causes for PPRs were diagnostic (30%), medication (27%) and management problems (27%). During the multidisciplinary meeting, the final decision on preventability changed in 11% of the cases. When a patient interview was available, it was used as a source of information to assess preventability in 26% of readmissions. In 7% of cases, the patient interview was mentioned as the most important source.
13% of readmissions were potentially preventable with diagnostic, medication or management problems being main causes. A multidisciplinary review approach and including the patient's perspective could contribute to a better understanding of the complexity of readmissions and possible improvements.
采用多学科方法,包括患者观点,确定出院后 30 天内计划性住院再入院的可预防程度、决定因素和原因。
前瞻性横断面单中心研究。
荷兰阿姆斯特丹的一家城市教学医院。
共纳入 430 例患者。纳入标准为:年龄≥18 岁,从参与的 7 个临床科室之一出院,出院后 30 天内计划性再入院。
参与科室的住院医师分别使用工具评估再入院是否由医疗保健引起、再入院的可预防程度以及可能的原因。此后,所有参与科室的住院医师和临床药师在多学科会议上讨论了可预防病例的可预防程度。主要结局是潜在可预防再入院的比例。次要结局是再入院的决定因素、可预防再入院的原因、多学科会议后可预防程度的最终决策变化以及患者访谈在评估可预防程度方面的价值。采用多变量逻辑回归分析潜在可预防再入院(PPR)和非 PPR 患者的特征差异。
430 例再入院中,56 例(13%)被评估为 PPR。年龄与 PPR 显著相关(调整后的 OR:2.42;95%CI 1.23-4.74;p = 0.01)。PPR 的主要原因是诊断(30%)、药物(27%)和管理问题(27%)。在多学科会议期间,11%的病例最终决策可预防程度发生变化。当可获得患者访谈时,将其作为评估再入院可预防程度的信息来源,占 26%。在 7%的病例中,患者访谈被认为是最重要的信息来源。
13%的再入院是潜在可预防的,主要原因是诊断、药物或管理问题。多学科审查方法和纳入患者观点有助于更好地理解再入院的复杂性和可能的改进措施。