Uitvlugt Elien B, Janssen Marjo J A, Siegert Carl E H, Kneepkens Eva L, van den Bemt Bart J F, van den Bemt Patricia M L A, Karapinar-Çarkit Fatma
Onze Lieve Vrouwe Gasthuis OLVG, Department of Hospital Pharmacy, Amsterdam, Netherlands.
Onze Lieve Vrouwe Gasthuis OLVG, Department of Internal Medicine, Amsterdam, Netherlands.
Front Pharmacol. 2021 Apr 13;12:567424. doi: 10.3389/fphar.2021.567424. eCollection 2021.
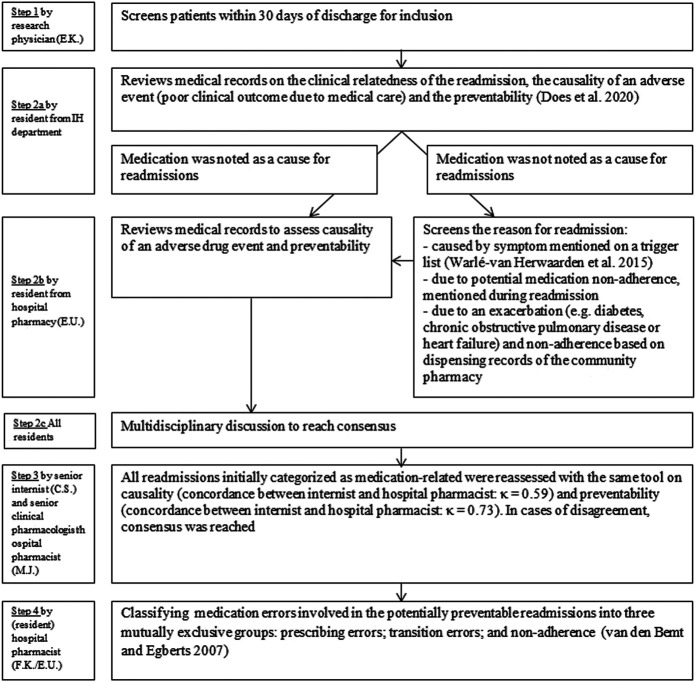
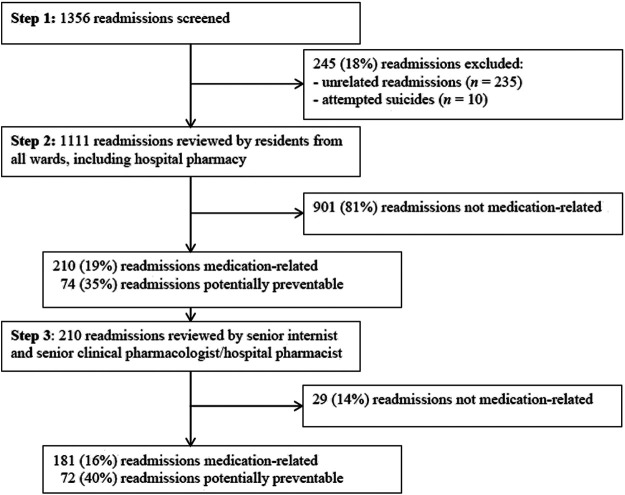
Hospital readmission rates are increasingly used as a measure of healthcare quality. Medicines are the most common therapeutic intervention but estimating the contribution of adverse drug events as a cause of readmissions is difficult. To assess the prevalence and preventability of medication-related readmissions within 30 days after hospital discharge and to describe the risk factors, type of medication errors and types of medication involved in these preventable readmissions. A cross-sectional observational study. The study took place across the cardiology, gastroenterology, internal medicine, neurology, psychiatry, pulmonology and general surgery departments in the OLVG teaching hospital, Netherlands. Patients with an unplanned readmission within 30 days after discharge from an earlier hospitalization (index hospitalization: IH) were reviewed. The prevalence and preventability of medication-related readmissions were assessed by residents in multidisciplinary meetings. A senior internist and hospital pharmacist reassessed the prevalence and preventability of identified cases. Generalized estimating equation with logistic regression was performed to identify risk factors of potentially preventable medication-related readmissions. Of 1,111 included readmissions, 181 (16%) were medication-related, of which 72 (40%) were potentially preventable. The number of medication changes at IH (Adjusted odds ratio [OR]: 1.14; 95% CI: 1.05-1.24) and having ≥3 hospitalizations 6 months before IH (ORadj: 2.11; 95% CI: 1.12-3.98) were risk factors of a preventable medication-related readmission. Of these preventable readmissions, 35% were due to prescribing errors, 35% by non-adherence and 30% by transition errors. Medications most frequently involved were diuretics and antidiabetics. This study shows that 16% of readmissions are medication-related, of which 40% are potentially preventable. If the results are confirmed in larger multicentre studies, this may indicate that more attention should be paid to medication-related harm in order to lower the overall readmission rates.
医院再入院率越来越多地被用作衡量医疗质量的指标。药物是最常见的治疗干预手段,但评估药物不良事件作为再入院原因的作用却很困难。本研究旨在评估出院后30天内与药物相关的再入院的患病率和可预防性,并描述危险因素、用药错误类型以及这些可预防性再入院所涉及的药物类型。这是一项横断面观察性研究。研究在荷兰OLVG教学医院的心脏病学、胃肠病学、内科、神经科、精神科、肺病科和普通外科进行。对早期住院(索引住院:IH)出院后30天内非计划再入院的患者进行了回顾。在多学科会议上,由住院医师评估与药物相关的再入院的患病率和可预防性。一名资深内科医生和医院药剂师对已识别病例的患病率和可预防性进行了重新评估。采用广义估计方程和逻辑回归来确定潜在可预防性药物相关再入院的危险因素。在1111例纳入的再入院病例中,181例(16%)与药物相关,其中72例(40%)可能是可预防的。索引住院时的用药变更次数(调整优势比[OR]:1.14;95%置信区间:1.05 - 1.24)以及索引住院前6个月内住院≥3次(ORadj:2.11;95%置信区间:1.12 - 3.98)是可预防性药物相关再入院的危险因素。在这些可预防性再入院病例中,35%是由于处方错误,35%是由于不依从,30%是由于转接错误。最常涉及的药物是利尿剂和抗糖尿病药物。本研究表明,16%的再入院与药物相关,其中40%可能是可预防的。如果这些结果在更大规模的多中心研究中得到证实,这可能表明应更加关注与药物相关的危害,以降低总体再入院率。