Department of Pharmacology and Molecular Therapeutics, Uniformed Services University of the Health Sciences, Bethesda, MD.
Department of Pathology, Uniformed Services University of the Health Sciences, Bethesda, MD.
Exp Hematol. 2020 Apr;84:54-66. doi: 10.1016/j.exphem.2020.03.004. Epub 2020 Mar 30.
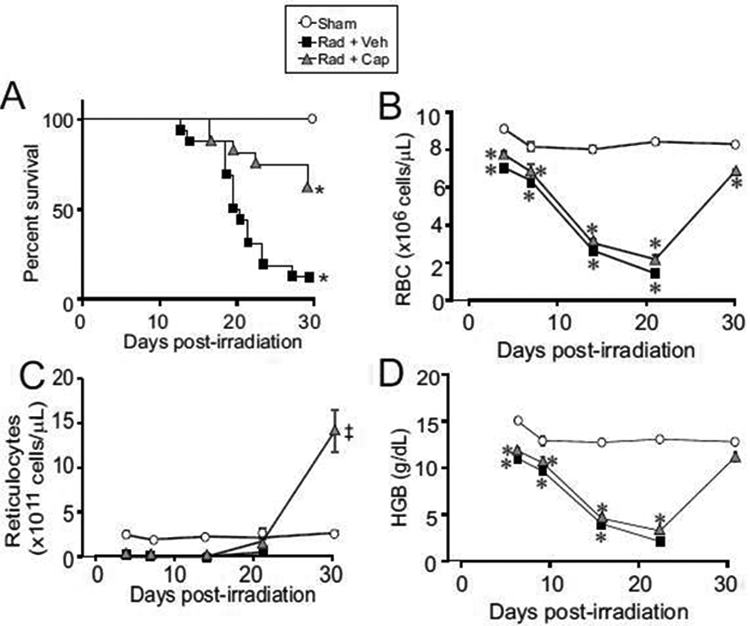
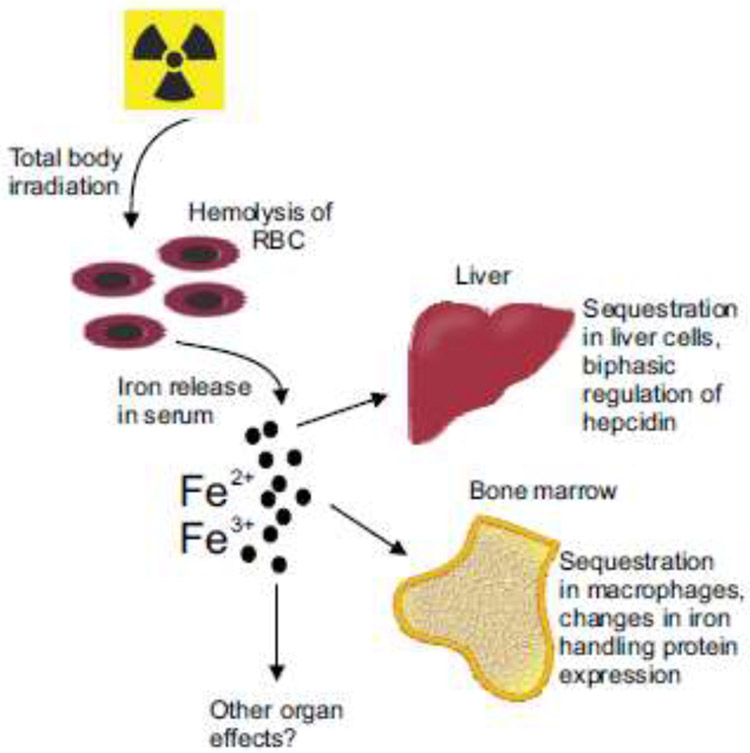
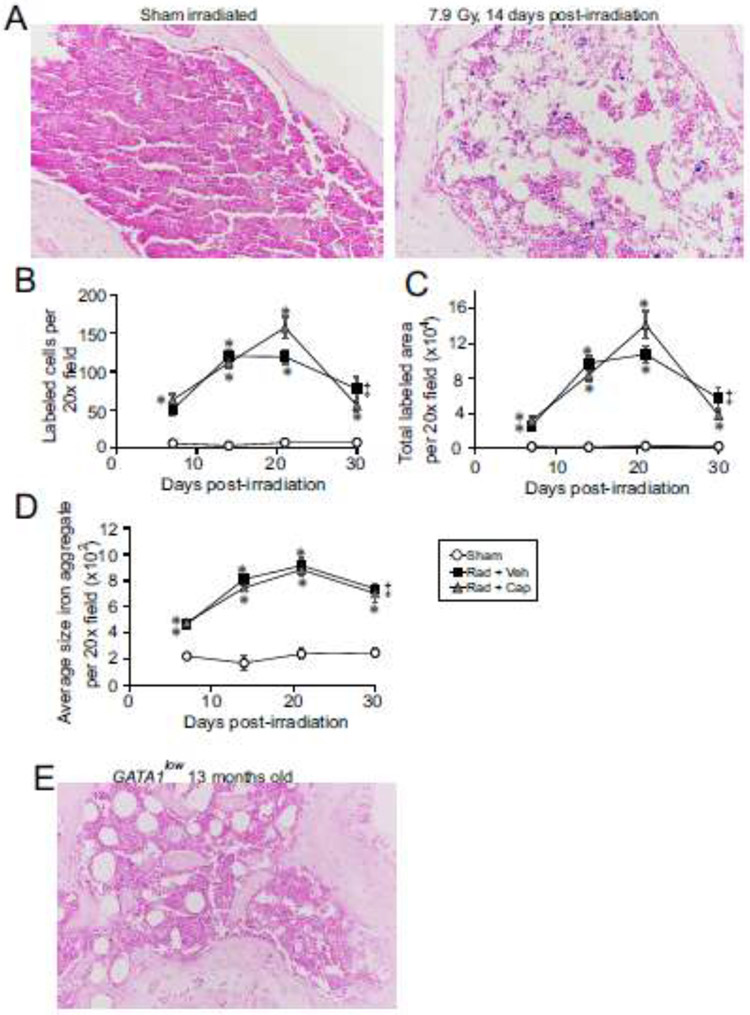
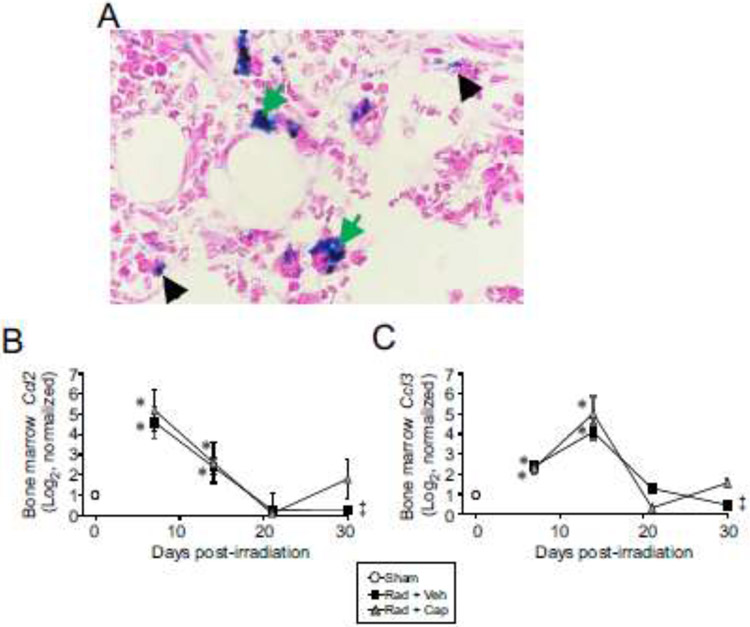
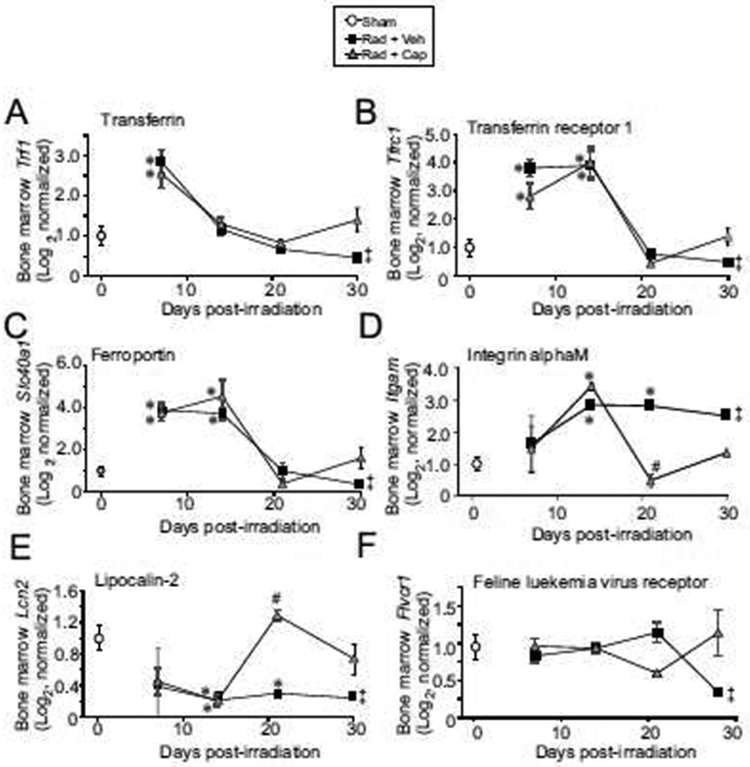
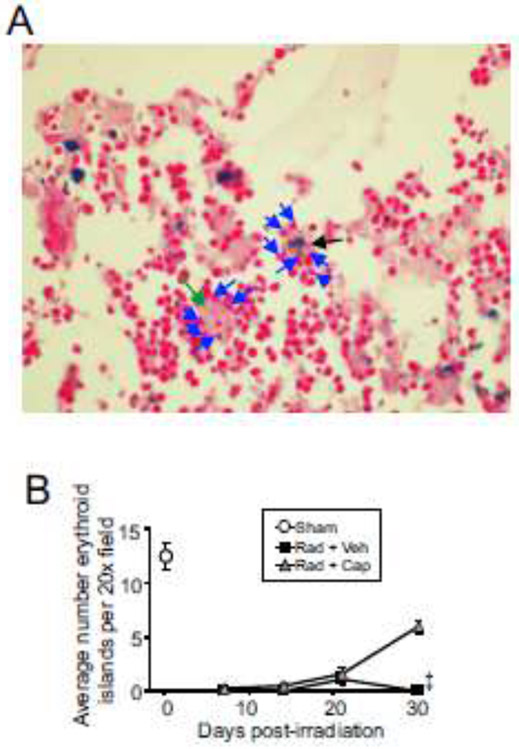
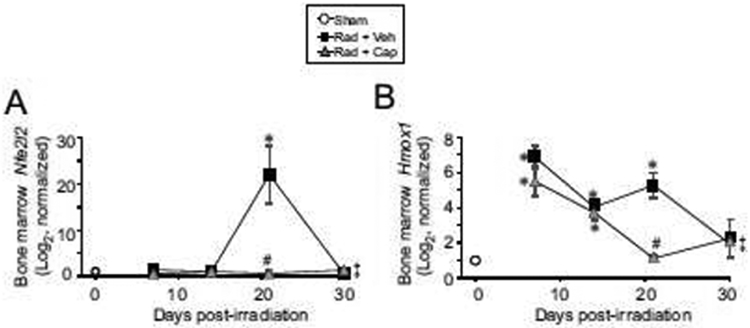
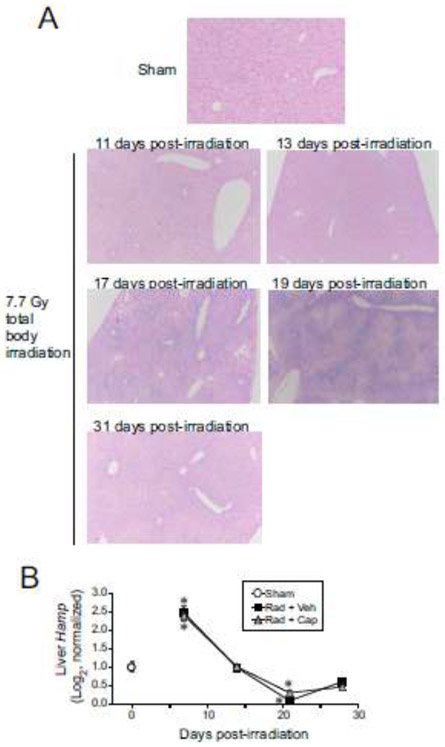
Exposure to high-dose total body irradiation (TBI) can result in hematopoietic acute radiation syndrome (H-ARS), characterized by leukopenia, anemia, and coagulopathy. Death from H-ARS occurs from hematopoietic insufficiency and opportunistic infections. Following radiation exposure, red blood cells (RBCs) undergo hemolysis from radiation-induced hemoglobin denaturation, causing the release of iron. Free iron can have multiple detrimental biological effects, including suppression of hematopoiesis. We investigated the impact of radiation-induced iron release on the bone marrow following TBI and the potential impact of the ACE inhibitor captopril, which improves survival from H-ARS. C57BL/6J mice were exposed to 7.9 Gy, Co irradiation, 0.6 Gy/min (LD). RBCs and reticulocytes were significantly reduced within 7 days of TBI, with the RBC nadir at 14-21 days. Iron accumulation in the bone marrow correlated with the time course of RBC hemolysis, with an ∼10-fold increase in bone marrow iron at 14-21 days post-irradiation, primarily within the cytoplasm of macrophages. Iron accumulation in the bone marrow was associated with increased expression of genes for iron binding and transport proteins, including transferrin, transferrin receptor 1, ferroportin, and integrin αMβ2. Expression of the gene encoding Nrf2, a transcription factor activated by oxidative stress, also increased at 21 days post-irradiation. Captopril did not alter iron accumulation in the bone marrow or expression of iron storage genes, but did suppress Nrf2 expression. Our study suggests that following TBI, iron is deposited in tissues not normally associated with iron storage, which may be a secondary mechanism of radiation-induced tissue injury.
全身大剂量照射(TBI)可导致造血急性放射综合征(H-ARS),其特征为白细胞减少、贫血和凝血功能障碍。H-ARS 导致死亡是由于造血功能不全和机会性感染。辐射暴露后,红细胞(RBC)因辐射诱导的血红蛋白变性而发生溶血,导致铁的释放。游离铁可能具有多种有害的生物学效应,包括抑制造血。我们研究了 TBI 后骨髓中辐射诱导的铁释放对骨髓的影响,以及 ACE 抑制剂卡托普利的潜在影响,卡托普利可提高 H-ARS 的存活率。C57BL/6J 小鼠接受 7.9 Gy、Co 照射,剂量率为 0.6 Gy/min(LD)。TBI 后 7 天内 RBC 和网织红细胞明显减少,RBC 最低点在 14-21 天。骨髓中铁的积累与 RBC 溶血的时间进程相关,辐射后 14-21 天骨髓中铁的积累增加了约 10 倍,主要在巨噬细胞的细胞质内。骨髓中铁的积累与铁结合和转运蛋白的基因表达增加有关,包括转铁蛋白、转铁蛋白受体 1、铁蛋白和整合素 αMβ2。辐射后 21 天,编码 Nrf2 的基因表达增加,Nrf2 是一种由氧化应激激活的转录因子。卡托普利并未改变骨髓中铁的积累或铁储存基因的表达,但确实抑制了 Nrf2 的表达。我们的研究表明,TBI 后,铁沉积在通常不与铁储存相关的组织中,这可能是辐射诱导组织损伤的继发性机制。