Department of Systems, Populations and Leadership, University of Michigan School of Nursing, Ann Arbor.
Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor.
JAMA Netw Open. 2020 Apr 1;3(4):e202044. doi: 10.1001/jamanetworkopen.2020.2044.
The strongest evidence for the effectiveness of Medicare's Hospital Readmissions Reduction Program (HRRP) involves greater reductions in readmissions for hospitals receiving penalties compared with those not receiving penalties. However, the HRRP penalty is an imperfect measure of hospitals' marginal incentive to avoid a readmission for HRRP-targeted diagnoses.
To assess the association between hospitals' condition-specific incentives and readmission performance and to examine the responsiveness of hospitals to condition-specific incentives compared with aggregate penalty amounts.
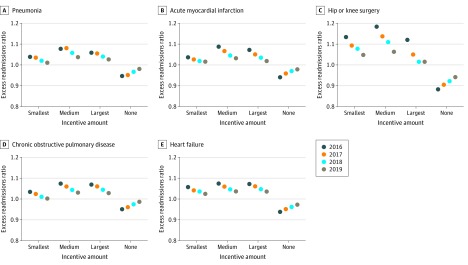
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort analysis used Medicare readmissions data from 2823 US short-term acute care hospitals participating in HRRP to compare 3-year (fiscal years 2016-2019) follow-up readmission performance according to tertiles of hospitals' baseline (2016) marginal incentives for each of 5 HRRP-targeted conditions (acute myocardial infarction, heart failure, chronic obstructive pulmonary disease, pneumonia, and hip and/or knee surgery).
Linear regression models were used to estimate mean change in follow-up readmission performance, measured using the excess readmissions ratio, with baseline condition-specific incentives and aggregate penalty amounts.
Of 2823 hospitals that participated in the HRRP from baseline to follow-up, 2280 (81%) had more than 1 excess readmission for 1 or more applicable condition and 543 (19%) did not have any excess readmissions. The mean (SD) financial incentive to reduce readmissions for incentivized hospitals ranged from $8762 ($3699) to $58 158 ($26 198) per 1 avoided readmission. Hospitals with greater incentives for readmission avoidance had greater decreases in readmissions compared with hospitals with smaller incentives (45% greater for pneumonia, 172% greater for acute myocardial infarction, 40% greater for hip and/or knee surgery, 32% greater for chronic obstructive pulmonary disease, and 13% greater for heart failure), whereas hospitals with no incentives had increases in excess readmissions of 4% to 7% (median, 4% [percentage change for nonincentivized hospitals was 3.7% for pneumonia, 4.2% for acute myocardial infarction, 7.1% for hip and/or knee surgery, 3.7% for chronic obstructive pulmonary disease, and 3.7% for heart failure]; P < .001). During the study period, each additional $5000 in the incentive amount was associated with a 0.6- to 1.3-percentage point decrease, or up to a 26% decrease, in excess readmissions (P < .001). Regression to the mean explained approximately one-third of the results depending on the condition examined.
The findings suggest that improvements in readmission avoidance are more strongly associated with incentives from the HRRP than with aggregate penalty amounts, suggesting that the program has elicited sizeable changes. Worsened performance among hospitals with small or no incentives may indicate the need for reconsideration of the program's lack of financial rewards for high-performing hospitals.
医疗保险住院患者再入院率降低计划(HRRP)有效性的最强证据涉及到接受处罚的医院与未接受处罚的医院相比,再入院率降低幅度更大。然而,HRRP 处罚并不是衡量医院避免 HRRP 目标诊断再入院的边际激励的完美措施。
评估医院特定条件激励措施与再入院表现之间的关联,并比较医院对特定条件激励措施的响应与总处罚金额。
设计、设置和参与者:本回顾性队列分析使用了来自参与 HRRP 的 2823 家美国短期急性护理医院的医疗保险再入院数据,根据 5 个 HRRP 目标条件(急性心肌梗死、心力衰竭、慢性阻塞性肺疾病、肺炎和髋部和/或膝关节手术)中每个条件的医院基线(2016 年)边际激励的三分位数,比较了 3 年(2016-2019 财年)的随访再入院表现。
使用超额再入院率来衡量随访再入院表现的平均变化,使用线性回归模型来估计基础特定条件激励措施和总处罚金额的变化。
在参与 HRRP 的 2823 家医院中,有 2280 家(81%)因 1 个或多个适用条件而有超过 1 次的超额再入院,543 家(19%)没有任何超额再入院。激励性医院减少再入院的平均(SD)财务激励从 8762 美元(3699 美元)到 58158 美元(26198 美元)不等,每避免一次再入院。与激励较小的医院相比,具有更大再入院回避激励的医院再入院率下降幅度更大(肺炎下降 45%,急性心肌梗死下降 172%,髋部和/或膝关节手术下降 40%,慢性阻塞性肺疾病下降 32%,心力衰竭下降 13%),而没有激励的医院超额再入院率则增加了 4%至 7%(中位数为 4%[非激励性医院的百分比变化为肺炎为 3.7%,急性心肌梗死为 4.2%,髋部和/或膝关节手术为 7.1%,慢性阻塞性肺疾病为 3.7%,心力衰竭为 3.7%];P < .001)。在研究期间,激励金额每增加 5000 美元,超额再入院率就会下降 0.6 到 1.3 个百分点,或者下降高达 26%(P < .001)。根据所检查的条件,回归均值解释了大约三分之一的结果。
研究结果表明,与总处罚金额相比,再入院回避的改善与 HRRP 的激励措施更密切相关,这表明该计划已产生了可观的变化。激励较小或没有激励的医院表现恶化可能表明需要重新考虑该计划对表现出色的医院缺乏经济奖励的问题。
