Testa Gianluca, Curcio Francesco, Liguori Ilaria, Basile Claudia, Papillo Martina, Tocchetti Carlo Gabriele, Galizia Gianlugi, Della-Morte David, Gargiulo Gaetano, Cacciatore Francesco, Bonaduce Domenico, Abete Pasquale
Department of Translational Medical Sciences, University of Naples "Federico II", Via S. Pansini, 80131, Naples, Italy.
Department of Medicine and Health Sciences, University of Molise, Campobasso, Italy.
ESC Heart Fail. 2020 Jun;7(3):1371-1380. doi: 10.1002/ehf2.12688. Epub 2020 Apr 3.
The assessment of frailty in older adults with heart failure (HF) is still debated. Here, we compare the predictive role and the diagnostic accuracy of physical vs. multidimensional frailty assessment on mortality, disability, and hospitalization in older adults with and without HF.
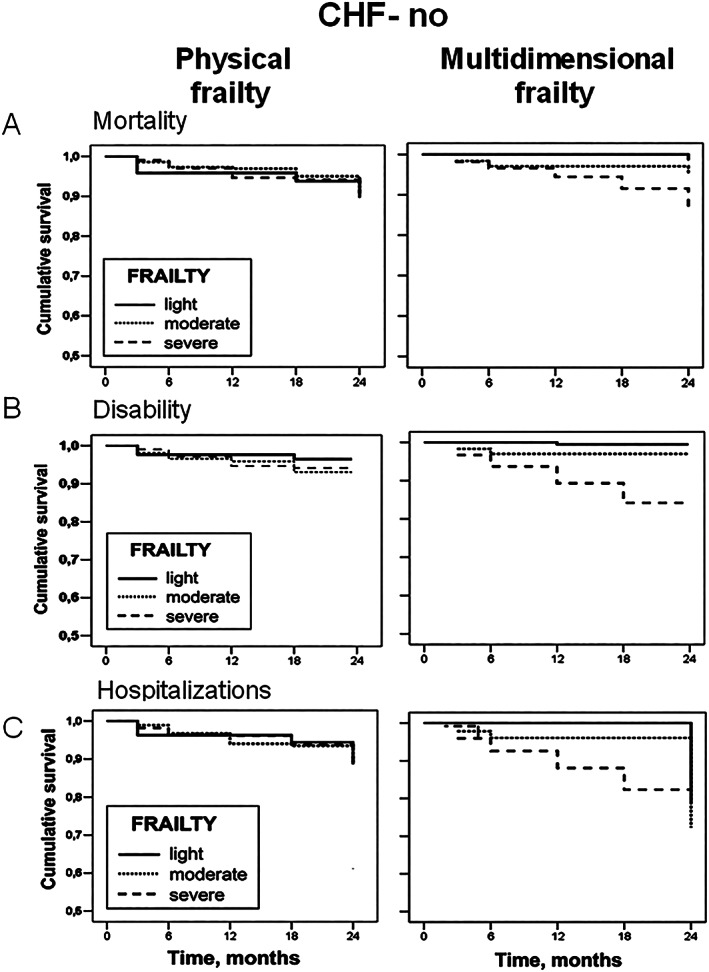
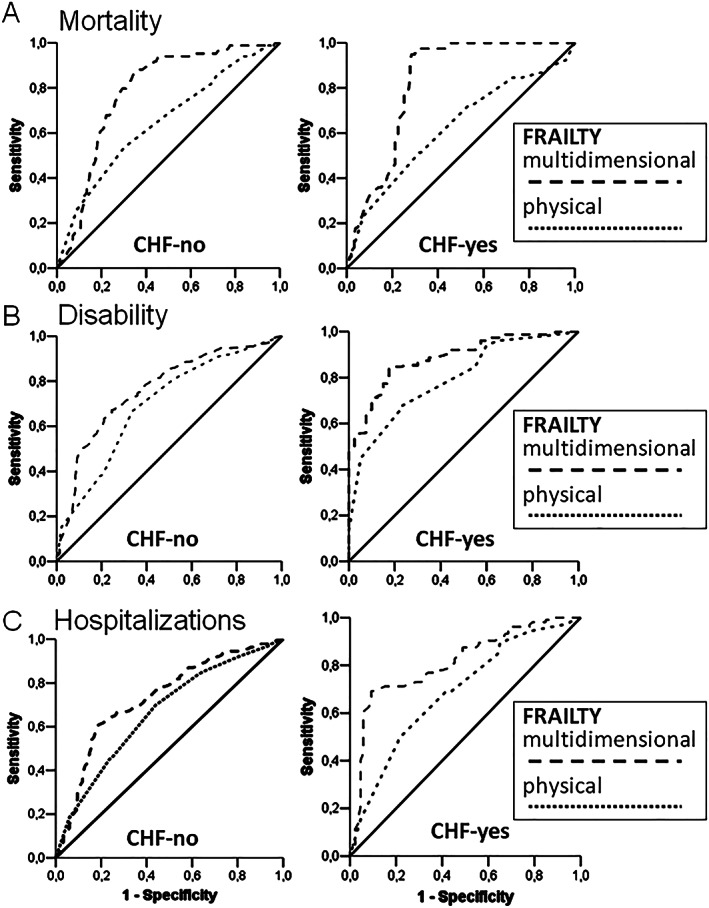
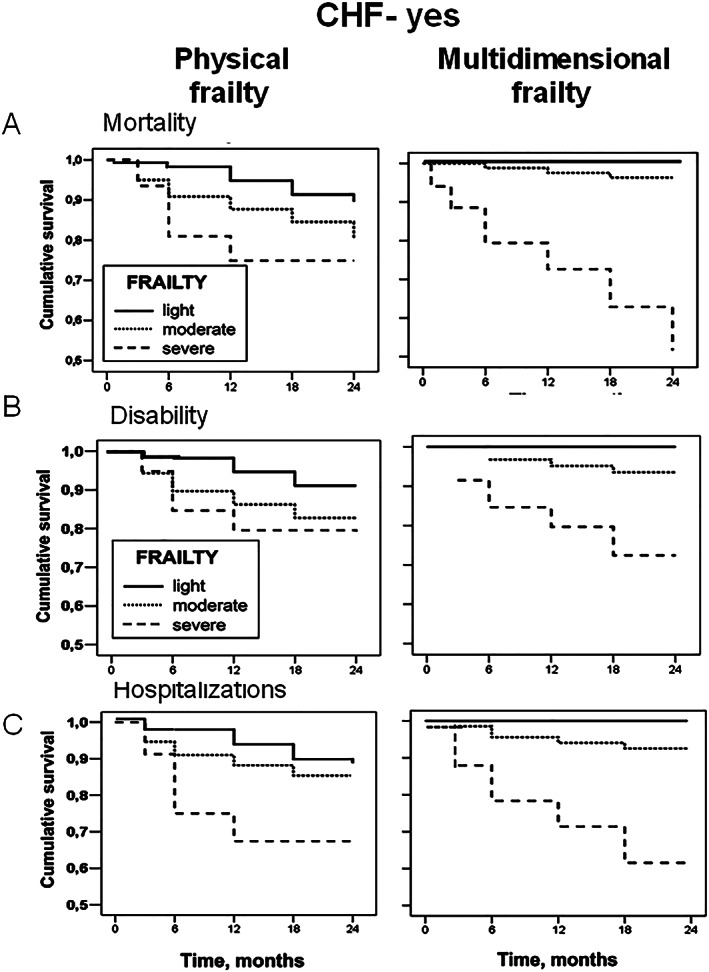
A total of 1077 elderly (≥65 years) outpatients were evaluated with the physical (phy-Fi) and multidimensional (m-Fi) frailty scores and according to the presence or the absence of HF. Mortality, disability, and hospitalizations were assessed at baseline and after a 24 month follow-up. Cox regression analysis demonstrated that, compared with phy-Fi score, m-Fi score was more predictive of mortality [hazard ratio (HR) = 1.05 vs. 0.66], disability (HR = 1.02 vs. 0.89), and hospitalization (HR = 1.03 vs. 0.96) in the absence and even more in the presence of HF (HR = 1.11 vs. 0.63, 1.06 vs. 0.98, and 1.14 vs. 1.03, respectively). The area under the curve indicated a better diagnostic accuracy with m-Fi score than with phy-Fi score for mortality, disability, and hospitalizations, both in absence (0.782 vs. 0.649, 0.763 vs. 0.695, and 0.732 vs. 0.666, respectively) and in presence of HF (0.824 vs. 0.625, 0.886 vs. 0.793, and 0.812 vs. 0.688, respectively).
The m-Fi score is able to predict mortality, disability, and hospitalizations better than the phy-Fi score, not only in absence but also in presence of HF. Our data also demonstrate that the m-Fi score has better diagnostic accuracy than the phy-Fi score. Thus, the use of the m-FI score should be considered for the assessment of frailty in older HF adults.
老年心力衰竭(HF)患者的衰弱评估仍存在争议。在此,我们比较身体衰弱评估与多维衰弱评估对有或无HF的老年人死亡率、残疾和住院情况的预测作用及诊断准确性。
共对1077名年龄≥65岁的老年门诊患者进行身体衰弱评分(phy-Fi)和多维衰弱评分(m-Fi)评估,并根据是否患有HF进行分组。在基线和24个月随访后评估死亡率、残疾和住院情况。Cox回归分析表明,与phy-Fi评分相比,m-Fi评分在无HF时对死亡率[风险比(HR)=1.05 vs. 0.66]、残疾(HR=1.02 vs. 0.89)和住院(HR=1.03 vs. 0.96)的预测性更强,在有HF时更是如此(HR分别为1.11 vs. 0.63、1.06 vs. 0.98和1.14 vs. 1.03)。曲线下面积表明,无论是在无HF(分别为0.782 vs. 0.649、0.763 vs. 0.695和0.732 vs. 0.666)还是有HF(分别为0.824 vs. 0.625、0.886 vs. 0.793和0.812 vs. 0.688)的情况下,m-Fi评分在死亡率、残疾和住院方面的诊断准确性均优于phy-Fi评分。
m-Fi评分在预测死亡率、残疾和住院方面比phy-Fi评分更优,不仅在无HF时如此,在有HF时亦是如此。我们的数据还表明,m-Fi评分的诊断准确性优于phy-Fi评分。因此,在评估老年HF患者的衰弱情况时应考虑使用m-Fi评分。